

| Contents | Previous | Next |
Prior to any discussion of interceptive orthodontic treatment, one must have a clear understanding of the general objectives of early orthodontic therapy. It was not too long ago that most clinicians waited until the permanent dentition had erupted before instituting orthodontic therapy. However, the dentist began to realize that most of their patients’ pre-pubertal growth had already taken place, and that orthopedic correction of any skeletal disharmonies was almost impossible to correct.(10) Also, leeway space, which is the difference in width between the deciduous molars and the smaller permanent premolars, could not be utilized after the exfoliation of the deciduous teeth, and any minor anterior crowding that existed could not be easily treated without saving this critical space. (18)(19) These and other considerations almost compelled the clinician to begin treating early, at least during the “mixed dentition.”
The objectives of early orthodontic treatment are as follows:
Attain Genetic Growth Potential
A pioneer in orthodontics, a student of Dr. Angle’s and a long-time professor at the University of Illinois, Dr. Alan Brodie, stated that a child’s facial growth pattern is established early in life, as early as the fourth month of age, and once established, the growth pattern of the individual can be easily predicted unless it is upset by some extrinsic factors.(20) In other words, the dental profession was told about growth prediction as far back as l94l. Once knowing what a child’s growth pattern is, and if it is deemed unsatisfactory, the clinician can utilize certain orthopedic devices, such as a headgear, to redirect the growth of the jaws to a more harmonious relationship. Therefore, it is dependent on the clinician to help the patient attain his or her growth potential with early orthodontic intervention.
Establish Normal Relationships
Teeth can be moved at any age, but there is only a short period during the age of a growing patient that a clinician can effect the growth of the jaws in order to obtain a normal maxillo-mandibular relationship. In other words, the spatial relationship between the jaws is the most important orthodontic treatment objective, no matter what the age of the patient. Whatever severe skeletal discrepancies are not treated with orthopedics during growth usually have to be corrected surgically in the patient’s adult dentition.
In a classic article in 1967, Dr. T. M. Graber and associates, explained to the dental profession the important differences between orthodontic and orthopedic forces, and it is the role of the clinician to utilize this information in order to treat his or her patient correctly.(21)
There are certain extrinsic factors that create functional interferences during growth. Such habits as thumb sucking and mouth breathing can create a narrow maxilla, when compared to the mandible, thus causing the lower jaw to deviate to one side or the other during occlusion. These types of functional interferences must be treated early, or the patient may suffer from various growth discrepancies of the jaws, or abnormal temporo-mandibular joint disfunctions. (22)
Maintain Normal Function
Before the clinician can hope to maintain normal function, he or she must know the difference between what is normal and what is abnormal for every stage of dental development. What may be normal at one age, may very well be abnormal for another age. The dentist must know the difference between “transient” and “incipient” malocclusions. Examples of the former are the aforementioned “ugly duckling” stage of dental development, the “end-to-end” or “flush terminal plane” relationship of the permanent molars in the “mixed dentition,” and the lingual eruption of the lower permanent incisor teeth. These examples are “normal” malocclusions at a particular age, and should be allowed to develop naturally without any orthodontic intervention. On the other hand, if the clinician sees that the patient is developing an “incipient” malocclusion, or one which is abnormal for a given age, then it is the dentist’s responsibility to intercept this malocclusion before it worsens.
As described previously, there is a certain eruptive sequence of the permanent teeth that should occur, which is different between the two jaws.(10) It is not so important that the patient follows his or her “calendric” development, as long as the permanent teeth are erupting in correct sequence. It is important to remember also that if a permanent tooth is erupting on one side of the dental arch, its “mirror image” tooth on the other side should also show evidence of eruption. If this does not occur, then the dentist should look for such problems as overly retained deciduous teeth, or even the congenital absence of permanent teeth.
There are three basic types of orthodontic treatment, namely, preventive, interceptive and corrective therapy.(10) The latter is mostly concerned with the permanent dentition where it is too late to institute preventive and interceptive procedures. Preventive orthodontics implies those procedures which the clinician can accomplish that would eliminate treatment in the future. Examples of these are: correct interproximal tooth restorations, timely exfoliation of primary teeth, and eliminating any extrinsic factors such as habits and mouth breathing which have an effect on the normal growth and development of the jaws.
Interceptive orthodontics is perhaps the most important procedure that a general dentist can perform in his or her important role as the “watch dog” of the dental profession. It is up to the clinician to differentially diagnose those cases that require proper interceptive procedures that can be readily treated by the general dentist, and to properly refer those cases to a specialist that require more intensive therapy. In other words, the dentist should be able to differentiate the “easy” cases from the “difficult” ones, and try and concentrate on the former. Examples of interceptive orthodontics are: orthopedic guidance of developing skeletal malocclusions such as Class II division l, Class II division 2 and Class III discrepancies. Certain anterior open bite malocclusions also fall into this category. However, the types of patients that usually can be treated very successfully by the dentist using interceptive procedures are those that have developed certain problems due to prolonged habits such as thumb sucking, as well as problems caused by extensive mouth breathing.
Dentists and parents have always been concerned with the psychological and physiological effects of infantile intraoral habits such as thumb sucking.(22) What causes some children to suck their thumb and others to completely ignore this digit? Is this a normal response or one that is garnished with present and future psychological problems? What types of physiological problems do thumb sucking cause, and are the results of this habit temporary or permanent? At what age should a “normal” child cease sucking his or her thumb? Should parents discourage their off-spring from any oral habits? What methods should be used to discourage the continuance of prolonged thumb sucking habits? Is professional help needed to do this, and if so, what kind? A psychiatrist? A pediatrician? A children’s dentist? A general dentist? An orthodontist?
To begin with, the “hand-to-mouth” cycle is normal for infants, and any attempt by parents to prevent their child from the inherent satisfaction that their child derives from this “habit” will create more harm than good. (Figure 90) Generally speaking, any intra-oral damage that most thumb sucking habits create is temporary and effects only the anterior portions of the jaws. Any interruption of normal development that this habit may create, however, depends on the so-called “trident of habit factors”.
Trident of Habit Factors
If a child sucks his or her thumb all day long, with a great deal of intensity, and especially if the habit is a prolonged one, the damage to the jaws can be permanent and affect even the posterior segments of the occlusion.
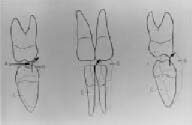
The greatest effect of a prolonged thumb sucking habit is to the anterior segment of the dental arch. The thumb protrudes the upper anterior teeth, and forces the lower anteriors lingually. An anterior open bite is created, and tongue thrusting develops in order for the patient to form an anterior seal during deglutition. The aforementioned signs are often referred to as a “thumb sucking malocclusion.” (Figure 91) If the habit is broken prior to 3 1/2 to 4 1/2 years of age, the above discrepancies are usually temporary. However, if the habit is allowed to progress past this age range, and especially if it is occurring concurrently with the eruption of the permanent incisor teeth, the damage can become more permanent, and may create a skeletal open bite as well as a Class II maxillo-mandibular relationship.
It is usually futile and unwise for a parent to force a child to stop a prolonged thumb sucking habit. Perhaps more harm than good can arise from this unwarranted discipline of the child. In most cases, some type of fixed appliance therapy by the dentist is required to help the patient in his or her first attempt in life at breaking a “bad habit.” (Figures 92 and 93) The optimal time for appliance placement is between the ages of 3 1/2 and 4 1/2 years, preferably during the spring or summer when the child’s health is at its peak, and sucking desires can be sublimated in outdoor play and social activities.
The “tongue crib” appliance serves several purposes. First, it renders the finger habit meaningless by breaking the suction that is created by the close proximity of the thumb and the hard palate. The child may place his or her finger in the mouth, but he or she gets no real satisfaction from it. Second, by virtue of its construction, the appliance prevents finger pressure from displacing the maxillary incisors further labially, creating more damage and causing a greater likelihood of abnormal tongue and lip function.
Third, the appliance forces the tongue backward, or at least prevents the tongue from thrusting between the upper and lower incisors in order to form a seal during the act of deglutition. If the patients are normal, healthy children, no unfavorable results are observed except for a temporary sibilant speech defect when the appliance is first placed, but disappears in a very short time.
|
|
|
| Figure 90. In-utero view of “early” thumb sucking pattern. | Figure 91. “Thumb sucking malocclusion” includes spacing, anterior open bite and spacing, protrusion of upper incisors and reclining lower incisors. |
Figures 94 through 96 illustrate a case that was originally misdiagnosed as a Class II skeletal open bite. After a thorough cephalometric diagnosis and patient history, it was determined that the patient had a typical thumb sucking malocclusion. This case was treated in a short period of time, about 4 to 6 months, with a single tongue crib appliance. Once the thumb habit was cured, the patient’s occlusion reverted to her hereditarily predetermined morphogenetic pattern, which was normal.
The real danger from a prolonged thumb sucking habit is the possible change to the occlusion, sufficient to allow the potent buccinator muscle forces to create a full-fledged malocclusion. It is these perverted forces that create the unilateral and bilateral crossbites so often associated with finger-sucking habits. (Figure 97) It must be kept in mind that the two halves of the maxilla are actively growing in width during the adolescent stages at which time thumb sucking habits are occurring. There is a discrepancy in width between the maxillary and mandibular dentition, and because of the narrowing of the maxillary arch, the patient is forced to shift the mandible to the left or right in order to create a “functional occlusion.” In other words, what appears to be a unilateral crossbite is in essence a bilateral problem. (Figure 98)
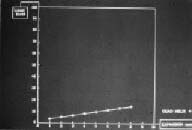
In this type of situation, an appliance should be designed to not only widen the buccal segments of the maxillary dental arch, but also to create a physiologic orthopedic force in order to position the two bones of the maxilla in a more normal relationship. It is the author’s opinion that the most “physiologic” appliance to use at this particular stage of growth and development is the quad helix appliance. (Figure 99) This appliance derives its name from the four helices that are incorporated in the 0.040" palatal wire prior to it being soldered to the bands that are eventually cemented to the maxillary second deciduous molars. The appliance is activated, or widened, a total of 8 millimeters prior to cementation. (Figure 100) Research by the author has determined that this amount of activation is sufficient to create an orthopedic effect on the developing maxilla and to treat most cross bites created by prolonged thumb sucking habits.(23)
 |
 |
| Figure 92. “Personalized” tongue crib. | Figure 93. Palatal view of tongue crib. |
 |
 |
| Figure 94. Side view of “thumb sucking malocclusion.” Note maxillary incisor protrusion and anterior open bite. | Figure 95. Palatal view of tongue crib used to treat prolonged thumb sucking and malocclusion. |
 |
 |
| Figure 96. Models of occlusion treated with tongue crib. | Figure 97. Apparent unilateral cross bite. Note the lower midline shift to patient’s left. This is a sign of a bilateral problem. |
Functional malocclusions should be treated as soon as they are seen in order to create the proper environment for the future development of the dentition. (Figure 101) This is a good example of performing a correct differential diagnosis of a transient malocclusion, which “treats itself” by normal growth and development, and an incipient malocclusion, which needs early intervention, such as the treatment of a functional malocclusion.(10) If this is not done, a functional malocclusion could develop into a more serious skeletal problem.
Fixed habit breaking tongue cribs are usually the method of choice, because they do not require patient compliance. If the patient is extremely motivated and cooperative, the clinician may attempt to utilize a tongue crib embedded into a modified Hawley type of removable orthodontic appliance. (Figure 102)
When a newborn infant attempts to swallow, he or she must thrust the tongue forward in order to create a seal for deglutition. (Figure 103) This is called “infantile” or “visceral” swallowing. As teeth erupt, the proximity of the anterior teeth act to create the seal for swallowing in the adult patient. (Figure 104) This is called “somatic” swallowing. If there is an anterior open bite and the front teeth are not able to approximate, the patient must then thrust the tongue forward in order to swallow, just as an infant does. (Figure 105) Since an average person swallows 900 to 1100 times per day, tongue thrusting can aggravate the anterior open bite problem. There are only a few circumstances in which the tongue causes the open bite syndrome, such as when a true macroglossia can affect the intraoral structures. (Figure 106) Generally speaking, the treatment described for a prolonged thumb sucking habit is usually the therapy of choice for tongue thrusting, unless the latter is due to an abnormal skeletal problem, which then needs extensive mechanotherapy. (Figure 107)
It is often thought that tongue thrusting is caused by the lack of breast-feeding of an infant. In other words, children that are extensively bottle-fed, the older nipples had too large of an opening, and the infant had to thrust his or her tongue forward to stop the excessive flow of milk. True or not, the manufacturers of artificial nipples altered the design to have smaller openings and more anatomically shaped.
The hyoid bone is often termed the “skeleton of the tongue.” This is because the supra-hyoid muscles extend from the base of the tongue to the hyoid bone. In a normal situation, the hyoid bone is found to be at a level between the third and fourth cervical vertebrae as seen on a lateral cephalometric radiograph. (Figure 108) If the patient has a true tongue thrusting problem, the hyoid bone will be found in a superior position, indicating to the clinician that more extensive therapy may be needed for this type of a patient. Often times, orthodontists will refer their tongue thrusting patients to a speech therapist, who will instruct the patient on proper swallowing and tongue position.
 |
 |
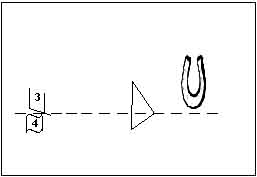
| Figure 98. Diagram showing the unilateral cross bite B), but when the midlines are aligned C), it is actually a bilateral cross bite. A) shows the mandibular shift to the patient’s left creating the “functional” malocclusion. | Figure 99. Quad helix appliance to treat narrow maxilla caused by prolonged thumb sucking habit. |
 |
 |
| Figure 100. Graph showing how 8mm of activation of the quad helix creates about 15 ounces of force, sufficient for widening the maxillary complex in children. | Figure 101. After about four months of treatment with the quad helix appliance. Note the midlines. |
 |
 |
| Figure 102. Tongue crib embedded in the palatal acrylic of a removable appliance. | Figure 103. Sagittal view of newborn infant illustrating a tongue thrust across the edentulous dental pads during swallowing. |
 |
 |
| Figure 104. As the teeth erupt and come together in the anterior region the incisors and canines form the necessary seal for deglutition. | Figure 105. An anterior open bite allows the tongue to come forward each time the patient swallows. |
 |
 |
| Figure 106. Skeletal open bite caused by macroglossia as a result of a lymphangioma of the tongue. | Figure 107. Tongue crib for the treatment of tongue thrusting. |
 |
 |
| Figure 108. Normal position of hyoid bone. | Figure 109. Nasal breathing warms, moistens and filters the air and allows for normal growth of jaws. |
Mouth Breathing
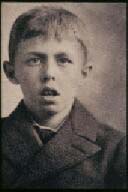
Nasal breathing is important, not only for health reasons, but also for the normal growth and development of the craniofacial complex. (Figure 109) The nose acts as a filter to clean, warm and moisten the air before entering the lungs. Mouth breathing does not allow the normal development of the maxilla because of the lateral pressure produced by the buccinator muscles on the upper jaw structure. Also, because the mandible is kept open during mouth breathing, there is a tendency for the posterior teeth to supra-erupt causing an open bite and an increase in the vertical dimension of the patient. In the early 1900’s Angle wrote about the importance of the nasal airway, and showed illustrations of various patients that he termed had a “mouth breathing syndrome.”(24) (Figure 110)
Adenoids
One problem that is definitely associated with tongue thrusting and mouth breathing is the proliferation of adenoid tissue. The normal nasopharynx includes the posterior wall of the nasal pharynx and the superior surface of the soft palate. (Figure 111) The normal “velo-pharyngeal” closure occurs between the nasal pharynx and the soft palate each time the patient swallows and speaks certain sounds. (Figure 112) The adenoid tissue is found at the posterior wall of the nasal pharynx and if proliferated, it can cause a blockage of the normally patent nasal airway. (Figure 113) This prohibits normal nasal breathing by the patient, encourages mouth breathing, and produces a malocclusion similar to that found in thumb sucking and tongue thrusting patients. In severe cases, not only does mouth breathing cause a narrowing of the maxilla, but it can interrupt the normal forward development of the mandible. (Figure 114) This is a perfect example of an extrinsic etiologic factor causing a malocclusion to develop, and is considered to be a major factor, even more important than intrinsic causes.
The treatment of proliferated adenoids is extremely controversial. Most physicians are reluctant to indiscriminately prescribe adenoidectomy, since lymph tissues act as an important defense mechanism for the body. Nevertheless, the dentist should consult with a physician to discuss the possibility of at least a partial adenoidectomy in severe cases that produce skeletal types of malocclusion. It is often incumbent upon the dentist to help instruct our medical colleagues about the importance of a patent airway and the role that hypertrophied adenoid tissues play in the underdevelopment of the maxillo-mandibular complex. It certainly aided the author’s relationship with his otolaryngology colleagues when he spoke to them several years ago about this important topic. It also helped our medical counterparts when research was performed to objectively determine the space available for proper nasal breathing using cephalometric analyses.(25)
 |
 |
| Figure 110. “Mouth breathing syndrome” as illustrated by Dr. Angle. | Figure 111. Nasopharynx. Note posterior wall of the nasal pharynx, where adenoid tissue is located, and the superior surface of the soft palate. |
 |
 |
| Figure 112. Normal velopharyngeal closure. | Figure 113. Lateral cephalometric view of proliferated adenoid tissue. Note small airway and malocclusion associated with mouth breathing. |
 |
 |
| Figure 114. Mouth breathing patient with anterior open bite and narrow maxilla. | Figure 115. Frontal view is best to measure width of nasal cavities. |
Since proliferated adenoid tissue can cause a tongue thrust due to an attempt by the patient to open the oral pharynx, the dentist should never place a tongue crib in cases of hypertrophied intra-oral lymph tissues. A patent airway is crucial prior to any type of orthodontic appliance therapy.
Nasal Cavities
Beside the pharynx, it is critical for the nasal cavities to also be patent for the patient to breathe through his or her nose. As mentioned previously, the nose warms, filters, and moistens the air prior to passage into the lungs. Therefore, the nose plays an important role other than just “cosmetics.” A deviated septum and hypertrophied turbinates may block the nasal cavities and cause mouth breathing. It is critical for the dentist to evaluate this area of breathing as well. There is no better way to diagnose true nasal breathing problems than to utilize a frontal cephalometric radiograph. (Figure 115) This view allows the clinician to evaluate the width of the nasal cavities and to denote any deviation of the nasal septum. Blockage of the nasal cavities is the most common reason for mouth breathing in adult patients, and surgical intervention by an otolaryngologist is a relatively easy procedure to correct this problem.