|
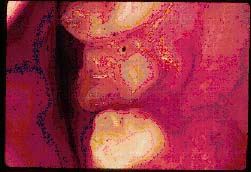
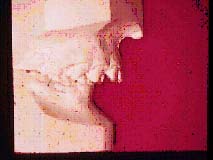
| Figure 16. Labioversion of mandibular incisor |
It is estimated that only 1% of the population has a "perfect" occlusion. Conservatively speaking, more than 20% of the population that has a malocclusion could benefit from some type of orthodontic treatment. Therefore, it is important for the dentist to determine which of those malocclusions he or she examines needs orthodontic treatment to prevent the occlusion from becoming "pathologic."
Although we want to treat each patient as an individual, and do not want to "pigeon hole" people into "groups," certain malocclusions have certain characteristics that are common. And, since the characteristics of each malocclusion are the objects that are treated, it is important to understand these as thoroughly as possible.
Also, by classifying something, it is easier to communicate certain information to the patients as well as to other members of our profession.
It is best to use the following order to classify occlusions:
v Individual Malpositions
v Horizontal and Vertical Relationships of Incisor Teeth
v Inter-arch Discrepancies
v Profile, Facial, and Dental Arch Characteristics
v Individual Malpositions
The classification of a malocclusion should begin with a detailed explanation of the malposition of each individual tooth in each dental arch. The term used to describe these malpositions is "version." Different types of versions are:
|
|
| Figure 16. Labioversion of mandibular incisor |

|

|
| Figure 17. Linguoversion of mandibular incisor | Figure 18. Palatal version of maxillary canine |
Linguo- or palatal version: This is a tooth that is misplaced to the lingual or palatal side of the dental arch. (Figures 17 and 18)

|
|
Figure 19. Mesioversion of maxillary first molar |
Mesioversion: This is when the tooth is displaced mesial to its normal position. (Figure 19)
Distoversion: This is when the tooth is displaced distal to its normal position.
|
|
Figure 20. Infraversion of ankylosed deciduous molar |
Infraversion: This is when a tooth has insufficiently erupted, such as a "high" canine or an ankylosed deciduous molar. (Figure 20)
Supraversion: This is when a tooth has erupted further than usual with reference to the occlusal plane.
Torsiversion: This is a tooth that is abnormally rotated either mesially or distally.
Transversion: This refers to the situation in which one tooth has displaced another, such as when a lateral incisor and canine are interchanged.
Of course, an individual tooth can be in several different "versions" at once. For example, a tooth may be in labio-, mesio-, supra-, and torsiversion at the same time.
Incisor Overjet (Horizontal Overlap)
|
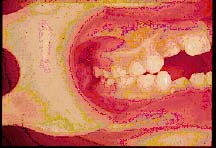
| Figure 21. Excessive horizontal overlap |
Certain malocclusions cause the maxillary incisor teeth to be positioned too far forward or too far behind their mandibular antagonists. When the upper incisors are protracted, this situation is referred to as an excessive "overjet" or horizontal overlap. (Figure 21)

|
| Figure 22. Anterior crossbite |
Incisor Overbite (Vertical Overlap)
 |
|
Figure 23. Excessive vertical overlap |
A normal overbite or vertical overlap is present when approximately 10% of the labial surface of the lower incisor is overlapped by the maxillary incisor. When either the maxillary or mandibular incisors over-erupt, the lowers are often partially or completely overlapped by the uppers. The patient is then said to have a "deep overbite," or excessive vertical overlap. The same situation would occur if the posterior teeth are infra-erupted. Figure 23
|
|
Figure 24. Anterior open bite |
Contrary to this situation, certain skeletal abnormalities or extrinsic factors often cause supra-eruption of posterior teeth or infra-eruption of the incisors. In such a case the incisor teeth do not approximate in occlusion. The patient is then said to have an "anterior open bite." (Figure 24)
This portion of occlusion classification was devised by Dr. Edward Angle in 1899(7). Since it is still being utilized today, it must have a great degree of merit. This classification assumes that the maxillary first permanent molar is in a correct position, because it is the "key" to this classification. It must be noted that Dr. Angle deter- mined this classification before cephalometric radiographs were developed, and therefore it is only a dental classification.
Class I
A Class I occlusion exhibits a well balanced muscle system, one which each clinician attempts to achieve as a final result of orthodontic treatment. It is important to note that all ideal occlusions are Class I, however all Class I occlusions are not ideal. A Class I malocclusion is associated with a normal maxillo-mandibular skeletal relationship; the discrepancy is between tooth and individual jaw size. In other words, the teeth are either crowded, or there is inter-dental spacing present.

|
|
Figure 25. Class I neutro-occlusion |
As in an ideal occlusion, in a Class I malocclusion the mesiobuccal cusp of the maxillary first permanent molar occludes in the buccal groove of the mandibular first permanent molar. This is also called a "neutro-occlusion." (Figure 25)
The skeletal and musculature relationships are ideal and harmonious in a Class I malocclusion, and except for the arch length-tooth size discrepancy, this type of orthodontic problem presents the fewest treatment complications if the correct mechanotherapy is performed. (Figure 26)
|
|
| Figure 26. Class I normal relationships |
A "sub-division" of a Class I occlusion is termed a "bimaxillary protrusion." This is normal and commonly observed in certain ethnic groups, where the dental, skeletal and muscular relationships are normal, but where the upper and lower dental arches are forward with respect to their bony bases.
Class II Division 1
|
|
| Figure 27. Class II division 1 disto-occlusion |
A Class II malocclusion exists when the mandibular first permanent molar is distal to its maxillary counterpart. This is also termed a "distoocclusion," because the lower molar is distal to the upper molar. (Figure 27) It may be the result of a retrognathic mandible, a protracted maxilla, or a combination of the two. If the Class II situation is skeletal in nature, then there is said to be a "basal" discrepancy, meaning that the positioning of the base of the mandible or maxilla are at fault. The exact etiology of a Class II division 1 discrepancy, however, can only be ascertained by a lateral cephalometric analysis.
Aside from the anteroposterior skeletal discrepancy, the arches may be crowded and an anterior open bite may also be present. Because of the "overjet" of the anterior segment of the dental arch in a Class II malocclusion, the lower anteriors are free to supra-erupt toward the palate, causing a deep overbite. If there is an "anterior tongue thrust," this will prevent the incisors from supra-erupting, and then an anterior open bite will develop.

|
|
Figure 28. Class II abnormal relationships |
Unlike the Class I occlusion, where a normal balance of muscle pressure exists, a Class II division 1 malocclusion exhibits abnormal musculature, often with hypotonic upper lip and hypertonic lower lip. (Figure 28) Because of the skeletal discrepancy and the muscle imbalance, the treatment of this malocclusion poses more treatment complications than do the Class I problems.
Subdivision. Often in certain Class II division 1 malocclusions, there is a situation where the occlusion is a Class I on one side and a Class II on the other. Then, it is classified as a "Class II division 1, subdivision left or right", depending on which side is Class II.
Summary of Class II Division 1 Malocclusions
� Overjet
� Deep Bite or Open Bite
� Basal Dysplasia
� Changed Muscle Function
Class II Division 2
|
|
| Figure 29. Class II division 2 incisor inclinations |
As in a Class II division 1 malocclusion, a division 2 also presents a disto-occlusion. This is the only relationship that the two discrepancies have in common. The typical Class II division 2 malocclusion is also characterized by a deep anterior overbite (vertical incisor overlap), lingual inclination of the maxillary central incisors, often labial tipped upper lateral incisors and an exaggerated curve of Spee in the mandibular dental arch with little or no crowding. (Figure 29)

|
| Figure 30. Class II division 2 vertical dimension |
The skeletal characteristics of this malocclusion more closely resemble a Class I situation than a Class II division 1 discrepancy. The growth potential of the mandible is favorable (in a forward direction), and there are no unusual problems with the perioral musculature other than the effects of the less than normal vertical dimension. (Figure 30)
Because of the favorable growth pattern, the prognosis of a Class II division 2 malocclusion is relatively favorable if treated at an early age. However, the prognosis worsens as the age of the patient increases due to the deep overbite problem and the concomitant temporomandibular joint syndrome often associated with the over-closure of the mandible.
Class III
|
|
| Figure 31. Class III mesio-occlusion |
A skeletal Class III malocclusion is due to an over-growth of the mandible causing a mesio-occlusion and a consequent anterior crossbite. (Figure 31) In some cases, the problem is further complicated by an insufficient or retracted maxilla. Other characteristics of a mandibular prognathism are labial inclination of the maxillary incisors and lingually tipped lower incisors.
|
|
|
Figure 32. Class III abnormal relationships |
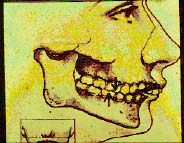
The tongue position is usually lower than normal and the lip tonicity is opposite to that found in a Class II division 1 occlusion. That is, in a skeletal Class III malocclusion, the upper lip is hypertonic while the lower lip is hypofunctional. (Figure 32)
If treated during the growth stage of an individual, orthopedic forces can be utilized to redirect the growth of the mandible, maxilla, or both. However, if allowed to develop to maturity, a mandibular prognathism usually requires a combination of orthodontic and surgical procedures to correct.
|
|
|
Figure 33. Convex, straight and concave profiles |
The facial profile of an individual is either straight, convex, or concave, depending upon the spacial relationship of the maxilla and mandible. (Figure 33) The Class I occlusion profile is straight. Because the mandible is retrognathic in a Class II malocclusion (especially a division 1) the profile is usually convex. A protracted maxilla would accentuate this situation. The opposite is true in a Class III malocclusion. The prognathic mandible and/or retracted maxilla produces a concave profile.
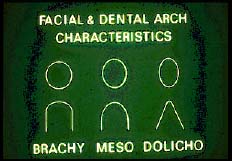
Facial and Dental Arch Characteristics (Figure 34)
|
|
| Figure 34. Facial types (above), dental arches (below) |
Mesofacial: A Class I occlusion presents with normal musculature and a pleasant ovoid facial appearance. The face is neither too long nor too wide and is associated with a similar jaw structure and dental arch configuration.
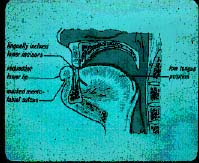
Dolichofacial: This type of face is long and narrow and is associated with either a Class II division 1 or a Class III malocclusion. The dental arches in these relationships are also narrow and may be associated with a "high" palatal vault.
Because of the narrow nasal airway in these patients, they are likely to be
"mouth-breathers" and cause a narrowing of the maxilla due to the abnormal forces placed
on the upper jaw structure by the buccinator musculature. Because these patients
keep their mouths open to breathe, there is a tendency for the posterior teeth to
supra-erupt causing the mandible to grow in a vertical direction and creating a skeletal open bite.
Also, due to the small mandibular ramus, the masseter muscle on these individuals
is also small, and the occlusal forces are weak. This may allow the posterior teeth
to erupt more than normal with a concomitant anterior bite opening. Because of
the skeletal and muscular imbalance associated with this facial type, the associated
malocclusions are the most difficult to treat orthodontically.
Brachyfacial: This facial structure is short and wide and is usually seen in a Class II division 2 type of malocclusion. The arch configuration associated with this facial type is also relatively broad and square.
Patients of this facial type are very rarely mouth-breathers because of the relatively wide nasal airway. The mandibles of this facial type are broad and "square" with a large masseter muscle and strong occlusal forces. Because of the latter, posterior teeth are often infra-erupted causing a skeletal "deep bite." Therefore, the mandible becomes "over- closed," and these patients are often prone to temporomandibular joint problems. Treated early, however, malocclusions associated with this facial type have a good prognosis due to favorable mandibular growth.
References
7. Angle EH: Treatment of malocclusion of teeth, 7th ed. Philadelphia, 1907, S.S. White Manufacturing Co.
![]()