|
|
| Figure 35. Downward and forward growth of facial bones |
Introduction
It is an oversimplification to say that a child's head and face become bigger with age. There is a confusion by some dentists as to the difference between the definitions of growth and development, often using these words as meaning the same. The word "growth" means an increase in size. The increase in the size of a growing child is obvious to everyone. On the other hand, "development" is defined as the "progress toward maturity." These are more subtle changes than growth, and the aging process of an adult is a good example of these "subtle changes." Some of the questions to be answered regarding growth and development are:
„ Do all the bones of the head and face grow at the same time?
„ Do the bones grow at the same rate?
„ What is the mechanism of craniofacial growth?
„ How does growth affect the jaws and dentition?
„ How are the principles of growth and development applied in the clinic?
Bone Growth
Before discussing facial growth, a basic understanding of the various mechanisms of bone formation should first be reviewed.
Endochondral: This is the type of bone formation that occurs in the long bones of the arms and legs. Cartilage forms the "pre-skeleton" first, which then gives way to bone formation. Endochondral types of bones are generally very hard and strong. None of the bones of the head and face are endochondral because, if they were, the head would be too heavy. Nature spared us this problem but, as it is, the average human head weighs about 14 pounds, the weight of a bowling ball! The only areas in the skull where cartilage is found are: the spheno-occipital synchondrosis; the spheno-ethmoidal synchondrosis; the nasal septum; the mandibular condyle. Note that the "cranial base," the divider between the face and brain, is made up of a dense endochondral bony structure. Perhaps this is nature's way of protecting the delicate brain from any trauma that may occur in the facial area.
Membranous: This type of bone formation does not have a cartilagenous precursor. The undifferentiated mesenchymal cells differentiate into osteoblasts and then into osteocytes and form bone. These bones are less dense and lighter than endochondral types of bones. The bones of the head and face consist of this type of bone formation. Nature has created a face that is less dense, and lighter for the patient to "carry" throughout his or her lifetime.
Surface Apposition: This theory states that bone is laid down on the outer surfaces of the various bones of the head and face, and this is the mechanism that causes them to increase in size. Clinically, the most important aspect of craniofacial growth is the direction of growth of the various bones of the head and face rather than their increase in size.
Endochondral: This theory states that the growth sites for this type of growth are at the various cartilagenous areas of the head and face. Namely, the spheno-occipital and spheno-ethmoidal synchondroses, the nasal septum, and the mandibular condyle. The growth in these areas literally forces the bones of the head and face to grow in a certain direction. If one wishes to pursue a more detailed explanation of this growth theory, he or she can be directed to the research efforts of Sarnat(8).
|
|
| Figure 35. Downward and forward growth of facial bones |
Sutural: This theory states that the connective tissue cells within the sutures (between two membranous bones) proliferate and causes the bones to be forced apart. Then, surface apposition occurs on either side of the suture which eventually closes this space. The sutures are directed in such a manner that the net direction of growth of the facial bones is downward and forward. (Figure 35) This theory was proposed by Scott in his research endeavors(9).
Functional Matrix: This theory was first discussed by M. Moss(10) from Columbia University. He states that each individual has a predetermined genetic growth potential for the size of the important matrices of the head and face. Some of these matrices are: the socket of the eye, the nasal cavities, the oral cavity, and the pharynx. According to Moss, the bones of the head and face grow to a certain size and shape around the matrices.
It is thought by most researchers that the head and face probably grow because of a combination of the above theories. The best text to read to derive a thorough understanding of craniofacial growth mechanisms is "The Human Face" by Enlow.(11)
Growth of Bodily Tissues (Figure 36)
|
|
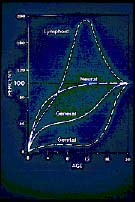
| Figure 36. Growth of bodily tissues |
Different tissues of the body grow at different rates and at different times. The neural tissue grows very early in life, and is well developed by the time a child is five years of age. Therefore, it is no wonder that a child at that age has the ability to learn and commence his or her schooling.
The lymphoid tissue also grows early, and even goes beyond the maximum limit of adulthood. Often this tissue proliferates to such a point that some has to be removed, hence the need for the removal of adenoids and tonsils. Adenoidectomies and tonsillectomies are not performed as frequently as in the past because of the lymph tissue's importance in the defensive mechanisms of a young child. However, in certain circumstances of nasopharyngeal obstruction causing mouth breathing and abnormal jaw development, orthodontists will refer their patient to an otolaryngologist for an evaluation for at least partial removal of the adenoid tissue.
The growth of the face closely resembles the general body growth curve. There is a specific growth spurt for boys and girls between the ages of 3 and 6 years. Often clinicians take advantage of this growth by using orthopedic appliances to correct severe incipient skeletal dysplasias. It is not unusual for a clinician to utilize orthopedic devices such as a head or neck gear for Class II cases and a chin-cup for Class III patients at this early age. These are perfect examples of early interceptive orthodontic treatment of incipient malocclusions.
After this early age, there is more or less a plateau in growth until puberty, during which time the general growth curve parallels the genital developmental curve. At puberty, the time of growth differs between males and females. For girls, this major growth spurt begins at 10 years of age and peaks between 11 and 13 years. For boys, maximum growth takes place between the ages of 12 and 16 years, with the peak around the ages of 14 and 15 years. Girls grow earlier than boys, therefore their orthodontic treatment should also precede that of boys if growth is to be utilized in the correction of malocclusions.
|
|
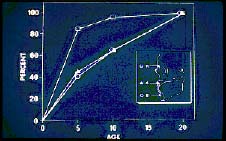
| Figure 37. Differential growth rate of head |
The different parts of the head also grow at different times. (Figure 37) Since the brain grows at an early age, it acts as a stimulant for the bones of the calvarium. This is the reason why young children look "top heavy," that is, the head looks bigger, proportionally, than the face and the rest of the body. The next part of the head to grow is the midface, since this is closest to the cranial base and brain. Because the midface is farther forward than the lower face, this gives a child a convex skeletal profile, similar to a mild Class II skeletal pattern. (This is a typical "transient" malocclusion that improves with normal growth.) The last region of the face to grow forward is the lower face or mandible. It finally catches up to the maxilla sometime between the ages of 10 and 15 years. The clinician can visualize the various skeletal problems that can arise if one or a combination of these three parts of the face grows abnormally.
References
8. Sarnat BG, Growth of bones as revealed by implant markers in animals, American Journal of Physiology and Anthropology, 29:255-286, 1968.
9. Scott JH, Growth at facial sutures, American Journal of Orthodontics, 42:381-387, 1956.
10. Moss ML: The functional matrix, in Kraus BS and Riedel RA (eds.): Vistas in orthodontics, Philadelphia, 1962, Lea and Febiger.
11. Enlow DH: The human face, New York, 1968, Harper and Row.
![]()