|
|
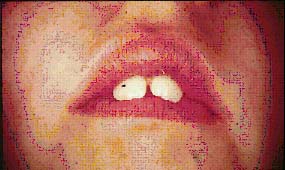
| Figure 1. Prolonged thumb sucking habit |
Why should the general practitioner be interested in orthodontics?
Orthodontics is a very rewarding aspect of dentistry. Unlike other fields of dentistry, the patient can visualize the results and is generally more appreciative of the clinician's accomplishments. There is no magic to orthodontics; in fact, moving a tooth is one of the easiest procedures to accomplish in dentistry. There is no reason why a general dentist cannot incorporate orthodontics into his or her practice as other specialties are incorporated. All it takes is a thorough understanding of the concepts of diagnosis, treatment planning and treatment.
One problem regarding orthodontic education in the dental curriculum is that it takes so long to treat a typical case, and therefore the results are not immediate. The contemporary dentist, however, has an advantage over his or her "older" counterparts. In the educational process of today, dental schools are "forced" into introducing the dental student to the clinical principles of orthodontics due to the curriculum requirements placed on them by the Council of Accreditation of the American Dental Association.
A study performed at the Great Lakes Naval Center in the 1940's showed that less than 1 out of 1,000 18-year old patients was caries-free. (That's almost 0%!) A more recent study by the National Institute of Dental Research found that approximately 50% of the 18-year old patients were caries-free. It is obvious that because of fluoridation and preventive dentistry, fewer patients have the amount of caries that were seen just a short time ago.
A study done by the NIDR in the early 1960's showed that more than 20% of patients in the 35-60 year old range were edentulous. A similar study in 1985-86 showed only 4% of that group were edentulous. Again, because of fluoridation and preventive dentistry, fewer patients are losing their teeth.
More patients are dying later in life, and with all their teeth, than ever before. As stated in a recent study: "....periodontal disease may fall as dramatically as has the prevalence of dental caries." There is a concerted effort today among periodontal researchers to develop chemotherapeutic agents to slow or arrest periodontitis, and even a future vaccine to eliminate it entirely. Nonetheless, present tartar control rinses and better periodontal care will more than likely eliminate periodontal disease as a cause of severe tooth loss in today's dental practices.
There is a very important role for the general dentist in orthodontic practice. The general practitioner/"orthodentist" should be able to perform an orthodontic diagnosis on all patients in his or her practice. Diagnosis and treatment planning are the "bread and butter" of orthodontics, because they answer most of the questions required of the dentist to understand the complexities of a malocclusion.
What are these important questions that should be answered by the "orthodentist" of the future?
Why? . . . Is the treatment needed, and for what purpose?
There are certain "transient" malocclusions that occur during various stages of dental development that are treated by "nature." In other words, these are "age-related" problems in which a malocclusion is "normal." Examples of these will be explained later in the text, and will be differentiated from "incipient" malocclusions, which occur at an early age but need clinical intervention. This is why "differential diagnosis" is the key to any orthodontic treatment plan.
When? . . . At what age should the treatment commence?
Not long ago, it was common practice to allow a child to develop his or her permanent dentition prior to the onset of orthodontic treatment. This mistake caused the clinicians of the past to rely on extraction of permanent teeth because growth was not a factor at this stage of development. Knowing what cases can be treated at an earlier age has allowed the clinician to "work" with growth and to aid in proper dental development.
What? . . . Is the problem skeletal or dental?
Oftentimes, a clinician will rely on a set of dental casts in order to determine the severity of a malocclusion. It will be shown that radiographic diagnosis is much more reliable than stone study models to determine the complexities of a malocclusion. Therefore, it is incumbent on the general dentist to determine the type of problem which the patient presents, and often this will determine whether the case is "easy," or one that needs to be referred to an orthodontic specialist.
Where? . . . Which direction should the teeth be moved?
An axiom in orthodontics used to be "never expand a dental arch." Another one was "never advance incisor teeth." These and other "myths" have long been discarded. However, a clinician must know his or her limitations as to the amount of expansion or incisor advancement a particular case can withstand and still remain stable after orthodontic treatment. Proper diagnosis and treatment planning provide the answers to the question, "Which direction should the teeth be moved?"
"How?" . . . Which appliance should be used?
Unfortunately, most general dentists try to answer this question first, and they "put the cart before the horse." In other words, the prior questions of why? when? what? and where? should be answered first before an attempt is made to design an orthodontic appliance. The immediate action to treat most likely comes from training received in dental school where a student reaches for his or her handpiece without much thought of differential diagnosis.
This is the process whereby the dentist determines the degree of difficulty of the orthodontic problem. The dentist then determines whether or not he or she has the ability to treat it; if it is too difficult, the patient should be referred to an orthodontic specialist. The best method to obtain a proper diagnosis, in any field of dentistry, is to have proper diagnostic records. Beside a detailed patient history and anatomically trimmed study models, the clinician requires the following radiographs for orthodontic diagnosis.
¨ Children
• Panorex radiograph to determine dental development, present and missing permanent teeth;
• Posterior bite-wings to determine caries;
• Lateral cephalometric radiograph to determine anteroposterior and vertical skeletal discrepancies;
• Frontal (P-A) cephalometric radiograph if an asymmetry is present.
¨ Adults
• Full mouth periapical and posterior bite wing radiographs to assess alveolar bone condition, root length, caries and other pathologic problems;
• Cephalometric radiographs if there are skeletal or asymmetric discrepancies.
Patient Analysis Case Selection
Only with a thorough understanding of the concepts of orthodontic diagnosis and treatment planning can the general dentist perform a proper patient analysis and case selection, and then to determine if the patient needs treatment and who should treat it.
| STAGES OF DENTAL DEVELOPMENT | ORTHODONTIC TREATMENT |
| Deciduous (2-6 yrs) ————— | Preventive |
| Mixed (7-12 yrs) —————— | Interceptive |
| Permanent (12+ yrs) ————— | Corrective |
A frequent question asked of an orthodontist is, "When should the clinician treat a malocclusion?" The author's usual answer to this question is, "Whenever the clinician diagnoses the problem." Although this may seem to be a sarcastic answer to some, the author's feeling is that often orthodontic problems go undetected leading to more complicated treatment "down the road." The general dentist is the "watch dog" of the dental profession, and should be able to detect all intraoral problems as soon as possible, treat those within his or her purview, and refer the more difficult treatment modalities to the specialist.
Another frequent question asked is, "When is the best age to perform routine orthodontic diagnosis on all patients?" The author's response to this question is, "As early as possible." As can be seen from the table above, preventive orthodontic care can only be accomplished in the deciduous dentition, between the ages of 2 and 6 years. Proper mesial and distal tooth restoration is important for the integrity of the dental arch, and the cessation of certain oral habits, such as thumb and finger sucking, should occur at this age to prevent dental and skeletal deformities from developing.
It is the author's opinion that every patient in the mixed dentition (ages 7-12 years) should have a thorough orthodontic diagnosis performed. This is the ideal age at which time certain dental and skeletal deformities can be intercepted with orthopedic and orthodontic appliances. The permanent teeth can be "guided" into the dental arch, and jaw growth can be "redirected" with the use of orthopedic appliances. The clinician can provide a great benefit to his or her patients by the use of interceptive techniques, allowing for ease of treatment and, in most cases, less costly therapy than allowing the malocclusion to develop into the adult dentition.
After the age of 12 years, most patients have all their permanent teeth, with the exception of their 3rd molars. Tooth guidance is impossible during the adult dentition, and more importantly, the major growth of the jaws has taken place by this age, and orthopedic appliance therapy cannot be performed effectively. Corrective orthodontic treatment is the only modality of choice for the clinician, and it usually requires fixed appliances and more complicated and costly treatment for the patient.
In order to appreciate what has been achieved in any area of dentistry, it is important to see how we got there and who helped us. In 1901, orthodontics was established as the first specialty in dentistry. Dr. Edward H. Angle "the father" of orthodontics, had both an M.D. and a D.D.S. degree. Born in Minnesota, he moved to St. Louis, and
started the first specialty program in orthodontics (Angle School of Orthodontics). His final move was to Pasadena, Calif. where he established his school, and taught numerous orthodontists who formed many of our contemporary concepts of orthodontics. He started the American Association of Orthodontists, as well as the American Journal of Orthodontics. He died in 1930, and "The Angle Orthodontist" and "The Angle Society" were formed in his memory, a prestigious journal and orthodontic society that are still in existence.
In 1900, Dr. Angle wrote his first textbook. In it, he wrote about the classification of malocclusion, and orthopedic and orthodontic appliances that are still used today.
„ Esthetics
„ Interception
„ Preprosthetics
„ Preventive Periodontics
„ Procedural
„ Prevention of Pathosis
„ Correction of Speech Defects
„ Facilitation of Surgery
„ Esthetics
Probably the greatest stimulus to seek orthodontic treatment is the unsightly appearance that is caused by malposed teeth. This is especially true when the esthetic appearance of the anterior region of the mouth is considered. Examples of these malocclusions are excessive flaring of the maxillary anterior teeth, diastema, anterior crossbites and anterior crowding.
|
|
| Figure 1. Prolonged thumb sucking habit |
„Interception
The interception of an incipient developing malocclusion by elimination of certain local factors over which the dentist has control is one of the most important reasons for early intervention with some type of limited appliance therapy. A good example of this purpose of orthodontic treatment is the interception of a thumb sucking habit during the "mixed" dentition. (Figure 1)

|
|
Figure 2. Preprosthetic appliance |
„ Preprosthetics
Often when teeth are not replaced for some time after extraction, the drifting that occurs can present a restorative problem. Closing and opening of spaces and uprighting of abutment teeth are often necessary before a proper removable prosthetic appliance can be fabricated. (Figure 2) Also, when teeth are moved into correct alignment prior to the use of fixed prosthesis, it is not necessary to remove excessive amounts of tooth structure.
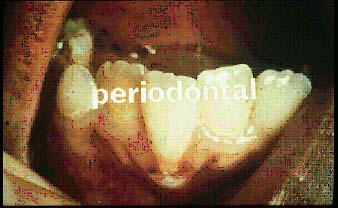
„ Preventive Periodontics
Much orthodontic therapy today can be termed preventive periodontics. The
periodontal reasons for orthodontic treatment are important for proper oral hygiene and for
the overall health of the dental alveolar structures. Often, as the result of an
arch-length deficiency, a mandibular incisor migrates into a position where the abnormal forces
of occlusion are detrimental to the surrounding periodontal structures. (Figure 3)
|
|
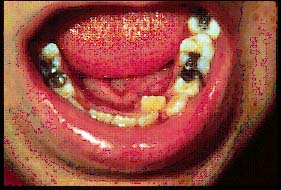
| Figure 3. Periodontically involved lower incisor |
In the resent past, an emphasis has been placed on adult orthodontic treatment. The periodontal implications of treatment are even more important for adults. Granted, orthodontic treatment may very well prevent future periodontal problems, but it is incumbent on the clinician to make sure that the adult patient's periodontal condition is "under control" prior to orthodontic treatment. The axiom "orthodontic treatment is a pathologic process from which the tissues recover" is especially important for the adult patient. As will be explained further, tooth movement is not a physiologic process, and the healthier the alveolar and periodontal tissues, the more likely the patient will "recover" from orthodontic treatment. It is the author's contention that every adult patient should undergo a thorough periodontic evaluation prior to any attempt of tooth movement.
|
|
| Figure 4. Procedural tooth movement |
„ Procedural
During the movement of a tooth, it may be necessary to shift adjacent teeth in order to gain sufficient space for the malposed or unerupted tooth. The creation of sufficient space for an unerupted or ectopically erupting maxillary or mandibular tooth is an example of this purpose of orthodontic treatment. (Figure 4)
„ Prevention of Pathosis
In some instances of severe protrusion of the maxillary anterior teeth, it is extremely difficult for patients to close their lips without a great deal of muscle strain. (Figure 5) The lips become extremely dry, with a resultant irritation. In some cases, anterior teeth are protrusive and unprotected, and can easily be fractured during an accident. Also, the tongue can become irritated if teeth are lingually or palatally displaced.
|
|
Figure 5. Protruding maxillary incisors |
„ Correction of Speech Defects
Certain malocclusions can cause defective pronunciation, especially of the sibilant sounds. The types of tooth malposition that can cause speech problems are anterior open bites, anterior crossbites, anterior tooth protrusion, interdental spacing, and interarch discrepancies. Because correct tongue position is often difficult to attain for proper speech and deglutition, correction by repositioning of the teeth makes it physically possible for the patient to pronounce the various sounds.

|
|
Figure 6. Facilitation of surgery |
„Facilitation of Surgery
The orthodontist and the oral surgeon work cooperatively as a team in the correction of such disorders as severe mandibular prognathism and cases of micrognathia associated with certain skeletal dysplasias. (Figure 6) This "joint effort" by the two specialists should commence prior to the onset of any treatment. After a thorough diagnosis, a treatment plan is formulated, and various fixed appliances are utilized by the orthodontist for presurgical orthodontic manipulations. The orthodontic appliances also aid the oral surgeon during the process of maxillomandibular fixation.
Prerequisites for Treatment
Certain limitations may rule out many cases in which it would be desirable to change the position of teeth but in which it would not be safe or practical to use "minor" procedures.
„ Adequate Space
„ Elimination of Interferences
„ Allowable Axial Inclination
„ Correctable Etiologic Factors
„ Favorable Periodontal and Periapical Prognosis
„ Absence of Contraindications
|
| Figure 7. Lower anterior crowding |
„ Adequate Space
There must be adequate space between the adjacent teeth to permit entry of the tooth that is to be moved, or it must be possible to gain the necessary room. Certain hereditary factors causing the patient to have small jaws and/or unusually large teeth can produce severe crowding and cause to contraindicate the use of removable orthodontic appliances. In most cases, these hereditary factors cause an arch-length, tooth mass discrepancy. (Figure 7) It is incumbent for the dentist to thoroughly understand the process and concepts of jaw growth and development. If the clinician realizes that the patient has a severe skeletal problem, then he or she should make the proper referral to a specialist for comprehensive treatment.
|
|
|
Figure 8. Bite plate appliance |
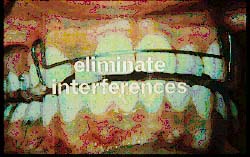
„ Elimination of Interferences
It must be possible to eliminate occlusal interferences in all excursions of the mandible at all stages of the tooth's movement into the desired position. The occlusions of anterior crossbites and deep overbites (incisor vertical overlap) have a tendency to cause interferences during the course of active tooth movement, and these interferences must be removed. Occlusal adjustments can be performed by the clinician during therapy, or the use of a removable maxillary bite plate appliances can be utilized. (Figure 8)
|
|
| Figure 9. Axial inclination of maxillary incisors |
„ Allowable Axial Inclination
Most minor tooth movement procedures produce a tipping action on the malposed teeth. The tooth to be moved must have such an axial inclination that the tipping forces used will not produce an unfavorable relationship. In other words, only "fixed" orthodontic appliances can cause the tooth to move "bodily," or in all planes of space. Therefore, prior to the use of removable appliances, the dentist must evaluate whether or not he for she can correct a malocclusion given the state of the labio-lingual or mesio-distal axial inclinations of the teeth. (Figure 9)
„ Correctable Etiologic Factors
All etiologic factors causing the malocclusion must be correctable. Some of these factors are extremely difficult to eliminate, but their continued presence will prevent successful treatment or retention of the orthodontic problem. "Intrinsic" factors are considered internal, and these include heredity and congenital deformities. Some of these factors may or may not be correctable, and they may cause the general dentist problems during the course of orthodontic treatment. The earlier these intrinsic factors are diagnosed, the sooner the dentist can realize the severity of the patient's problems in order to make an educated referral to a specialist for orthodontic treatment.

|
|
Figure 10. Nasopharyngeal airway |
On the other hand, "extrinsic" factors, as the word indicates, are external in nature, and are easier to control by the clinician after a proper diagnosis is made. Examples of these factors are prolonged intraoral habits such as thumb sucking, and mouth breathing. The latter may or may not be the result of a habit, but due to an internal problem such as hypertrophied nasopharyngeal adenoid tissue in a child. (Figure 10) It is important for the dentist to make this particular diagnosis, or perhaps refer the patient to an otolaryngologist for a medical review of any problem that exists.
„ Favorable Periodontal and Periapical Prognosis
Periodontal and periapical prognosis of the tooth must be favorable. The periodontium must be healthy in order to have the proper tissue response required for tooth movement. Too much emphasis cannot be placed on what was mentioned earlier, namely, "Orthodontic treatment is a pathologic process from which the tissues recover." Scaling, root planning and curettage are done before orthodontics, whereas most periodontal surgical procedures should be performed after orthodontic treatment. Endotherapy should be done before orthodontic therapy, as a vital tooth is necessary to prevent any possibility of root resorption during its movement.
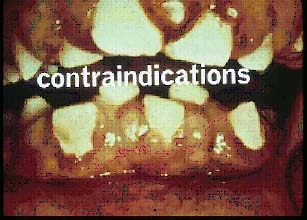
„ Absence of Contraindications
Systemic conditions that have oral manifestations must be ruled out prior to orthodontic tooth movement. Any factor that produces gingival enlargement can cause pressure that may force teeth to migrate. Systemic factors such as diabetes and patient reaction to certain medications can cause the intraoral tissues to hypertrophy, which would cause an impediment to tooth moving procedures. (Figure 11) A most important issue is good patient cooperation. Poor oral hygiene during the course of orthodontic treatment can also cause the gingival tissue to become irritated and often enlarged.
|
| Figure 11. Hypertrophy of gingival tissues |
Biomechanical Principles
Definition: "The application of the principles of mechanics to biologic systems." The topic of biomechanical principles cannot thoroughly be discussed in a few simple paragraphs. In fact, there have been several text books(1,2) written to adequately describe this most important aspect of orthodontic therapy. However, it is important for the clinician to realize that "the tooth does not know what appliance is being used on it." During the use of a removable orthodontic appliance, the pressure applied to a tooth by the round wire of the appliance is at one point of the tooth. As mentioned previously, it is not possible to produce "bodily" tooth movement–only tipping (labiolingual, buccolingual, and mesiodistal). Fixed appliances, on the other hand, can cause a tooth to move in all planes of space. Depending on the fixed appliance used, such sophisticated procedures as intrusion, rotation, extrusion and torque can all be accomplished. Again, numerous texts(3,4) have been written on the subject of fixed orthodontic appliances in order for the general dentist to get a thorough understanding and respect for this method of therapy.
| Force Systems | ||
| grams | forces | tooth movement |
| 0-100 | very light | little |
| 100-250 | light | effective |
|
250-500 |
heavy |
effective/multiple |
| 500+ | very | heavy none (orthopedic) |
Biology of Orthodontic Tooth Movement
|
|
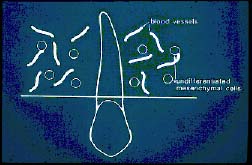
| Figure 12. Undifferentiated mesenchymal cells |
Prior to force: Undifferentiated (mesenchymal) cells (Figure 12)
|
|
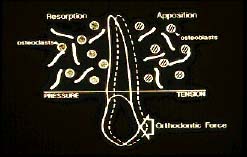
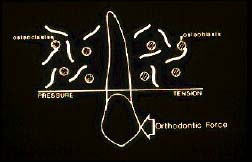
Figure 13. Osteoclasts and osteoblasts |
Orthodontic force: Pressureside: osteo clasts (resorption)
Tension side: osteo blasts (apposition) (Figure 13)
|
|
| Figure 14. Orthodontic force = tooth movement |
Causes tooth movement (Figure 14)
|
|
|
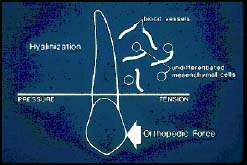
Figure 15. Orthopedic force = hyalinization |
Orthopedic force:
Heavy force causes force: "hyalinization" cell-free area on pressure side–no tooth movement– forces transmitted to distant craniofacial structures and causes orthopedic correction (Figure 15)
*For optimum tooth movement, use less force on an adult as compared to a child, because the adult has a diminished blood supply, and hyalinization can occur with heavy forces.
The above is by no means a complete description of the biology of orthodontic tooth movement. Again, the dentist should refer to the classic text books(5,6) on this subject to fully understand this most important aspect of clinical orthodontics. Nevertheless, the clinician can utilize the above summarized information to understand that light forces move teeth, and heavy forces prevent efficient tooth movement. This is contrary to what most consider logical thinking, that the more the force that is applied to a tooth, the more the tooth will move. It is most important to remember that the older the patient, the lighter the tooth moving forces should be.
A dentist may think that an adult's alveolar bone structure is "harder" than a child's, therefore more force is required to move an adult tooth. Contrary to this thinking, a heavier force on an adult is more likely to produce "hyalinization," or, a "cell free" area, incapable of any osteoclastic activity and bone resorption. On the other hand, if the clinician's goal is to use a child's tooth as an "anchor," as is the case during headgear therapy and the need for orthopedic force transmittal, then "heavy" forces should be used to accomplish this task.
References
1. Reitan K: Biomechanical principles and reactions. In Graber TM, Swain BF: Orthodontics: current principles and technique, St. Louis, 1985, Mosby-Year Book.
2. Chaconas SJ: Biomechanics in pre-restorative orthodontics. In Caputo AA, Standlee J: Biomechanics in clinical dentistry, Tokyo, 1995, Quintessence Co.
3. Thurow RC: Atlas of orthodontic principles, St. Louis, 1970, C.V. Mosby Co.
4. Proffit, WR: Contemporary orthodontics, St. Louis, 1993, Mosby-Year Book.
5. Norton LA, Burstone CJ, editors: The biology of orthodontic tooth movement, Boca Raton, FL, 1989 CRC Press.
6. Graber TM: Orthodontic principles and practice, Philadelphia, 1972, WB Saunders Co.
![]()