| Contents | Previous | Next |
by William M. Carpenter, DDS, MS; Peter L. Jacobsen, PhD, DDS;
and Lewis R. Eversole, DDS, MS, MA
Abstract: This article describes two approaches to the classification of oral mucosal lesions. One is based on the etiopathogenesis of the lesion and the second on the clinical appearance. These two approaches are compared and contrasted, and their integration is described. Combining these two classification schemas allows an excellent understanding of the various lesions so than an expeditious and correct diagnosis can result. Appropriate management and treatment can then follow.
The establishment of a differential diagnosis for lesions of the oral mucosa is often problematic. This problem relates to the large number of lesions that may affect a patient and the fact that many occur only rarely. A systematic approach to nosology is crucial. Classically, oral pathology has been taught following the etiopathogenic approach. This approach, as most commonly used in general pathology, considers the basic disease processes or mechanism and the body’s response, along with the etiologic factors involved. To approach the classification of disease from this viewpoint is efficacious and allows for effective management decisions. Once the etiology is understood, the treatment can be instituted.
General pathology texts are usually divided into chapters on inflammation and immunology, neoplasia, genetic and developmental disorders, and diseases of the various organ systems (e.g., cardiovascular, gastrointestinal, and liver).l-3 Oral pathology texts traditionally follow this same approach and include other categories specifically relating to oral lesions, such as odontogenic cysts and tumors, and salivary glands.4-9
The general etiopathogenic categories can be condensed into four major areas that can be best remembered by the acronym MIND (M = metabolic, I = inflammation, N = neoplastic, D = developmental diseases). This mnemonic reminds the student and practitioner to use his or her MIND to arrive at a correct diagnosis. This approach is condensed and simplistic but provides a good starting point for cerebration and further amplification of this classification10. The MIND classification system can then be expanded.
Although most but not all areas of etiopathogenesis are included here, this simplified system will allow a quick and easy review by the practitioner as the four major areas are considered. This system lends itself well to cognitive retention because one learns mechanisms of disease that are mentally imprinted as pictures, that occur as links. Learning the underlying basis of disease this way involves cellular processes in conceptional learning and is far more cognitively retentive than memorizing long lists.
| Table 1. The Mind Classification System
Metabolic (systemic)
Inflammatory
Neoplasia
Developmental
|
The practitioner must then be able to recall the signs and symptoms of the various categories of disease as a pertinent medical history and physical examination are performed. Age, sex, race, and gender may be important factors in data collection. The medical history would include questions regarding the chief complaint, history of present illness (lesion), past medical history, social history, and family history. The lesional history should include duration, pain, periodicity, treatment, and location. As this data is collected and tabulated, various diseases will be considered and deductive reasoning employed.
Physical examination of the head, neck, oral cavity, and particularly of the lesion is then carried out, and several aspects of the lesion must be taken into consideration. The visual assessment and palpation of the lesion of the oral mucosa would include an evaluation of any surface changes in the normal color or texture, along with any alterations in the normal morphology, including swellings, blisters, and/or surface ulcerations. These clinical categories are seen in Table 2. Several oral pathology textbooks now include a clinical outline section.
Setting aside the etiopathogenesis approach to disease classification for a moment, one must consider more practical clinical classification schemes. The categories that follow represent the various tissue alterations or lesions that clinicians observe.
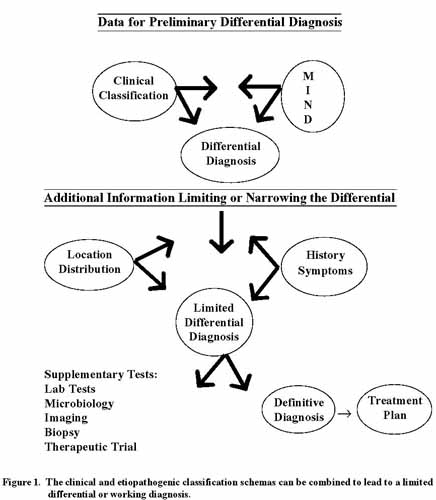
The clinical classification approach to differential diagnosis of oral soft tissue lesions can be correlated with histopathologic findings. As discussed for each clinical group of lesions, this correlation will allow the clinician to visualize and understand what is occur clinician integrates the clinical and etiopathogenic classification schemas, the various lesions become mentally manageable. Therefore a combination of these two approaches, if performed correctly, will lead to a limited differential or working diagnosis (Figure 1).
In general, the first step is to place the disease in one of the clinical appearance or lesional categories and then entertain thoughts as to which diseases present with such an appearance, while subcategorizing them as metabolic, inflammatory, neoplastic, or developmental. It may be necessary at this time to perform a supplementary diagnostic test to better delineate the definitive diagnosis. This test may be microbiological, serological, biochemical, imaging modalities, or therapeutic trial or may include a tissue sampling procedure (biopsy). Often a biopsy is necessary to establish the final diagnosis. However, occasionally a biopsy is unnecessary such as for a positive radiographic finding in an amalgam tattoo, a positive candidal microbiological test, or a positive serologic test for syphilis in a mucous patch. Once the definitive diagnosis has been established, the clinician can then administer the proper treatment. The final consideration is follow-up and re-assessment. This is a very important step that allows for there-establishment of normalcy and ensures that a correct diagnosis was achieved and proper treatment rendered.
Table 2. Lesions of the Oral Mucosa (Clinical Classification)
|
William M. Carpenter, DDS, MS, is professor and chairman in the Depart- ments of Pathology and Medicine at the University of the Pacific School of Dentistry.
Peter L. Jacobsen, PhD, DDS, is director of the Oral Medicine Clinic at the UOP School of Dentistry.
Lewis Roy Eversole, DDS, MSD, MA, is a professor of pathology and medicine at the UOP School of Dentistry and a head and neck pathology consultant to Pathology Consultants of New Mexico.
Copyright CDA Journal. Vol. 27. No. 8. August 1999
Reprinted with permission