| Table 2. Advantages and Perceived Disadvantages of Digital Radiography | ||||||||||||||||||||||||||||||||
Advantages
Perceived Disadvantages
|
By Dale A. Miles, BA, DDS, MS; Robert P. Langlais, DDS, MS; and Edwin T. Parks, DMD, MS
Abstract: Digital imaging is here. It is cost effective and helps dentists glean more useful information to make treatment decisions. Many more choices of digital systems are available for dentists to adopt than when the technology was introduced. The hardware is less costly than it was even one year ago, and image storage is now very inexpensive. Technical time is reduced, and no special training is required if the dentist or auxiliary has used a paralleling system.
Insurance companies are gearing up to accept image files attached to claims. Why, then, are dentists not buying these systems as fast as manufacturers can build them? This article explores that question and discusses the false assumptions behind perceived obstacles.
This article presents some basic information on charge coupled devices (CCDs), complimentary metal oxide semiconductor (CMOS) receptors and photostimulable phosphors (PSPs). It identifies available systems, reasons for acquiring this technology, and several perceived obstacles slowing the widespread adoption of digital imaging by dentists.
Also included is information on digital panoramic radiography and its potential impact on expediting dentists' acceptance of digital X-ray technology into their practices.
Whether they realize it or not, most dentists have probably used some form of digital imaging. Fax machines, intraoral cameras, and home video cameras use digital technology. Digital video discs (DVDs), also called digital versatile discs, are being advertised and presented as the next major digital media technology to affect the consumer. Some dentists have already purchased such a system. And, some of the more sophisticated practices are already looking to achieve their dental images film or digital on CD-ROM or DVD. All of these devices or systems are forms or digital technology.
A CCD is an imaging sensor, a solid state detector. It is a silicon chip with an embedded circuit that is capable of receiving X-rays (or light rays in a video camera system) and storing them briefly before transmitting the information by electronic signal to a computer monitor for display of the image. The electronic signal is just a wave or curve that is sampled along its length so that the computer can assign a digital number directly proportional to the amplitude of the wave at a given point. The conversion of this analog electric signal to a digital
Figure 1. In this example, the gray level 40 might relate to the image density of the enamel, while gray level 60 represents the density of the gutta percha. There is not much difference in the density of these two materials. The amalgam would have a density value or gray level number of 255 the brightest. Black would be 0.
number is called analog to digital conversion. Each digital number assigned corresponds to a particular density level or gray level of that area of the object that was imaged. Most images to be displayed on a computer monitor have 256 gray levels. Even though manufacturers claim 10 to 12 bit gray level image acquisition (1,024 to 4,096 grays), their systems can only display 8 bits/pixel of gray information (256 grays). The human eye can distinguish about 64 grays. Figure 1 explains this process. A more thorough explanation can be found in several previously published articles. l3
CCDs or CMOS receptors are also used in devices that can scan images, such as hand or desktop scanners. These devices allow a conventional film radiograph to be placed in a flatbed scanner, which captures a digital image of the radiograph. The image is only as good as the original film scanned. The production of this type of image is "indirect" because it is a secondary image scanned from the original. Some video camera manufacturers will tell you that you can make digital X-rays from their camera systems by pointing the camera at a film on a view box and capturing a picture of the X-ray. This is a poor technique and usually results in an inferior image because of inadequate illumination from the view box and trying to capture the image through the film base of the X-ray. Unless the original image is of high diagnostic quality and one uses a desk-top-type scanner with a "transparency mode" specifically designed for transilluminating the image, a good image will not be produced, at least not as good as acquiring it directly by using CCD-based systems.
| Table 1. Current CCD-Based Digital X-Rays Systems | ||||
|
Company |
Product Name |
Thickness (mm) |
Resolution (lp/mm) | Dose Reduction (vs. D-speed) |
| Schick Technologies | CDR | 5.0 | 9-10 | 80-90% |
| TreXtrophy Radiology | RVGui | 6.95 | 22 | 90% |
| ProVision | Dexis | 8.8 | 12 | 90% |
| DMD | MPDx | 3.2 | 22 | 90% |
| DentX | Sens-A-Ray 2000 | 6.0 | >15 | 90% |
| Cygnus Imaging | Cygnus Ray 2 | 5.0 | 12 | 90% |
| Planmeca | DIXI | 5.0 | 12 | 90% |
| Siorona | Sidexis | ? | ? | 90% |
| Welch Allyn | Reveal | ? | ? | 90% |
A direct digital image is one produced by the various commercial digital X-ray systems using a CCD as the image receptor (Figures 2a through c). Table 1 lists current systems and manufacturers. The device consists of several layers of silicon with an embedded circuit for capturing electrons produced when the X-rays exiting the patient strike a surface layer of amorphous silicon and break a bond in the material. For every bond broken, an electron is released. These electrons are then captured in a positively charged "well" (called the electron well) for a few microseconds before an electronic "gate" (the embedded circuit) is opened and the number of electrons in each well is read out as an electronic signal. l3 The signal is proportional to the number of electrons in each well and accurately represents the density at a specific point or region of the object that was X-rayed. The resultant digital image is an extremely accurate representation of the anatomic region that was imaged.
Table 2 lists both the advantages and perceived disadvantages of CCD-based digital systems. The advantages are obvious. This discussion will be limited to the disadvantages that seem to be the major obstacles to the widespread adoption of digital radiography by the profession.
| Table 2. Advantages and Perceived Disadvantages of Digital Radiography | ||||||||||||||||||||||||||||||||
Advantages
Perceived Disadvantages
|
The two most common types of solid state detectors available to dentists are the CCD and the CMOS sensors. Welch Allyn makes a sensor using a charge induced device (CID), but there is very little data about this sensor. Both CCD and CMOS devices were invented in the 1960s, along with the transistor. Neither the CCD nor CMOS device had the commercial viability that the transistor did at that time because the computer had not yet been developed sufficiently.
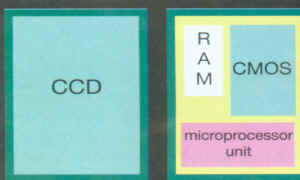
CMOS chips are used in every computer. They can be made cheaper than CCD chips because the manufacturing process is very mature. As yet, CMOS detectors have not been adequately tested for X-ray image capture. CMOS chips contain some RAM operation circuitry and a microprocessor on the same silicon chip (Figure 3). Thus, the noise level may be greater with CMOS sensors than with CCD because of electronic "crosstalk" between the elements. Also, because there are multiple components on the same chip, there is less sensor area available for image capture. This could mean less image information in an X-ray system. CMOS detectors appear to be more suited for commercial products such as digital cameras. Table 3 outlines the advantages and disadvantages of these sensors in terms of their technical specifications.
|
|
|
|
Figure 2a. A CCD image from Cygnus Imaging (CR2). |
Figure 2b. A CCD image from ProVision (Dexis) |

|
|
| Figure 2c. A CCD image from Schick Technologies (CDR). |
Figure 3. CCD and CMOS chips. |
PSP Technology
Photo stimulable phospor technology may be an interim imaging modality. While the plates are wireless and the technique digital, image acquisition is still a two-step process. The plates can be processed quicker than film, but there is still a significant waiting period between image acquisition and image display. The cost of the systems is more expensive initially than CCD or CMOS systems.
The phosphors in the plate enter into an excited state proportional to the X-ray exposure; but, unlike conventional screen phosphors (for example, panoramic screen/film combinations), PSPs do not immediately fluoresce to produce light photons. They only store the image information like the latent image in film based radiography. The receptor plates are scanned in a device by a laser that excites the phosphor to give up its stored light. This light emission is captured as an electronic signal and converted to a digital image (analog to digital conversion). The digital image can then be viewed on a monitor in about 5 � minutes, the time varying from the size or number of films being scanned. Image resolution is much less than with CCD receptors and ranges from 6 line pair/mm to 9 1p/mm depending on the product.
On the other hand, PSP receptors are not as sensitive to exposure time variations as film. They have an extremely wide exposure latitude; that is, they can be exposed to a wider range of exposure times and still be capable of displaying the information usefully. At about 1.6 mm, PSP plates are the same thickness as film.
Three manufacturers offer imaging systems that use PSP plates: Soredex (Helsinki, Finland, Digora), Digident (Israel, CDDent), and Gendex (Milwaukee, Wis., DenOptix).
| Table 4. Comparison of Approximate Costs of Initial Imaging Systems | ||
| Items | CCD | Film |
| Initial | ||
| X-ray tube | 3,500 | 3,500 |
| Darkroom | 6,000 | 0 |
| Computer/sensor | 0 | 7,995 |
| Film processor | 3,500 | 3,500 |
| Printer | 0 | 799* |
| Film duplicator | 600 | 0 |
| Film or paper | 1,500 | 1,500 |
| Film mounts | 500 | 0 |
| Film chemistry | 500 | 0 |
| 17,500 | 13,794 | |
| Ongoing | ||
| Film or disc costs/year | 800 | 35 |
| Technical time for image acquisition and procession | 5,040** | 2160+ |
| Technical time for maintenance | 192 | 0 |
| 4,352 | 1,475 | |
| After Year 1 Total | 27,884 | 17,464 |
| Savings | 10,420 | |
|
* It may not be necessary to purchase a printer for "hard copy" if the dentists plan to view the images on the monitor and store them electronically. ** All of the tasks related to film imaging involved substantial "tech time,"
the cost of which is related to the auxiliary. Film cost based on an average of 15 FMX series per week for 48 weeks and
a salary cost of $12/hour. Each FMX series was estimated to take 20 minutes to obtain images and 15 minutes to process
and mount. Annual tech time for film=420 hours; annual tech time for CCD=180 hours.) + Each digitally acquired series is estimated to take 15 minutes to acquire. There is no processing or mounting. |
||
There are many articles and publications that describe the wide array of advantages of digital imaging. l3 Perhaps the biggest advantage from the list in Table 2 is patient education and care. The excitement and professional acceptance regarding the intraoral camera is obvious. One of the reasons is because a picture is worth a thousand words. In many cases, the picture is worth a thousand or more dollars. Is the technology used only to generate more revenue for the dentist? In a sense the answer is yes. However, if the video camera or, in this case, the digital radiographic image can be used to explain a problem more precisely to the patient, and the patient is educated as to his or her disease state, then, of course, the patient is more likely to accept the explanation and the treatment. This results in more revenue. This is no different than when dentists try to show patients carious lesions on bitewing radiographs on a view box to educate them regarding an interproximal lesion. They usually can't see it. It would be helpful to be able to display lesions on a 19" monitor so patients can discern them for themselves (Figure 4). Why, then, are dentists not rushing to buy CCD digital radiographic systems? There are many reasons.

|

|
| Figure 4. An artist�s rendering of a "miniaturized" X-ray unit placed within the grasp of the dentist or dental auxiliary. | Figure 5. A CCD panoramic image. |
As much as dentists may not want to spend several thousand dollars on a new imaging device, they must examine the need for making the change very carefully. There are initial costs with both film based and digital systems. Table 4 is a gross comparison of the initial and ongoing costs for the first year of setting up either system. Dentists have darkrooms and use film daily and that initial cost has already been made up; but the advantages of consistency of image quality, rapid access to the images, and the ability to store them electronically and transmit them immediately by telephone more than justify the transition. The savings in office space and technical time for image acquisition and processing are also very strong arguments to switch. All imaging in the graduate Department of Endodontics at Indiana University School of Dentistry is taken with CCD sensors, stored in a computer, and written onto CDROMs weekly. All predoctoral dental and dental auxiliary students (both hygiene and assisting) have preclinical and clinical training in digital imaging. The move to digital imaging is inevitable.
As Table 3 shows, the initial costs of setting up a digital system, with all the advantages listed, are probably less than those of a standard film based, darkroom dependent radiographic system. In addition, the ongoing costs, in terms of technical time, are far greater with film than with digital radiography.
Other Obstacles
There are five additional obstacles that have impeded the progress of CCD imaging in the dental office. They are:
Lack of familiarity and use of computer based imaging technology, especially electronic image processing;| Ergonomic designs that are inappropriate for dentists and staff; | Workflow needs and equipment size in the existing operatory space; | Lack of training using advanced technology for evaluating diagnostic data: and | Lack of an imaging software interface with true clinical functionality. | |
Lack of Familiarity and Use
In general, people resist change. But, dental professionals must accept change, especially when it will improve the quality of patient care. Because dental schools in North America are just now beginning to adopt digital technology into their curricula, training in this area must be done through dental continuing education by individuals with educational backgrounds, rather than manufacturer's representatives. Much of the training can be done electronically, with basic instruction for dentists and staff being placed on CDROMs or DVDs for in office training. The programs would offer continuing education credits for both auxiliaries and dentists. In office training could be done as a training day set aside in the practice. Interactive Web sites will also be used to provide digital training and practice using image processing software.
Ergonomic Concerns
Where will this technology fit in the average dental operatory? Where does one put the computer, monitor, printer, video camera, and digital X-ray unit? One of the most cumbersome but necessary operatory tools is the X-ray tubehead. It has to be mounted on a wall, using up valuable space. Not everything can go on a mobile cart, which is difficult to navigate around the operatory, patient, and chair. The following two ideas could be useful to save valuable shelf, wall, and countertop space, and perhaps save money:
| Wireless transmission of the image or other data to the computer or monitor; | |
| A remote printer linked to the computer but in a central location; and | |
| A lightweight, portable X-ray generator to replace other tube heads within easy reach of the operator. |
Work Flow Needs
As just discussed, in most dental offices operatory space is at a premium. The X-ray machine takes up space because of the necessity for the heavy, cumbersome X-ray arm that is wall mounted. If the X-ray unit could be "miniaturized" and placed within the grasp of the dentist or dental auxiliary, operatory space would be preserved, and the procedure itself would become more attractive and efficient. This scenario improves the workflow. Figure 4 demonstrates this concept.
Lack of Training
Despite the advances in radiology available to the dentist, X-ray practices in the average office remain archaic. Courses in technology as old and widely adopted as panoramic radiology still draw rooms full of dentists and staff members who confide that they have never received formal instruction in the principles of panoramic imaging.
Manufacturers often succeed in bringing technology to the dentist well in advance of the dental training and education that would be useful to have in order to use the technology to its fullest advantage.
There are very few courses in oral and maxillofacial radiology that contain any digital imaging instruction. Thus, dental professionals are dependent upon the retailers of these systems for their training. This is, at best, an inadequate and possibly biased method of training, not because the manufacturers don't try their best to educate dentists about their systems, but because they cannot teach the principles of the imaging modality�only the technique or application. Yet, for most dentists, the instruction they and their staff receive is from a sales representative with no formal dental radiology training. Without understanding the system and its principles, the dentist will be very reluctant to switch to digital imaging from film-based imaging.
Software Interfacing
Until recently, manufacturers of imaging peripherals such as video cameras and digital X-ray systems, created their own, proprietary software unique to their hardware. Now they realize they must integrate imaging software with patient management software. The dentist does not want to have to close out a task such as a patient appointment when he or she wants to look at that patient's images.
Also, all charting software is still approached as a schematic representation and only indirectly reflects the true patient status. What is needed is a graphic constructed from the specific data for the patient (bone levels, soft tissue levels, etc.) of the clinical and radiographic findings that is accurate and interactive. For example, when a user clicks on a feature on the patient's panoramic image, such as a restoration, the program should automatically bring up or display the periapical radiograph of that region for better detail and diagnosis. It would also be convenient to be able to "map" a panoramic image precisely to the clinical findings, so that the clinical chart would be a customized, anatomically correct version of the patient's bone status. That could be done with digital technology, and it would better reflect the way a dentist actually practices.
Even as dentists continue to debate the advantages of digital intraoral radiography for their offices, manufacturers of radiographic equipment develop new technology. Several X-ray companies have introduced panoramic machines with CCD technology, which are capable of producing outstanding images (Figure 5). Planmeca Inc., of Wood Dale, III, received FDA approval for its machine, the DIMAX, in August 1997 and began receiving purchase orders immediately. The CCD digital upgrade can be retrofitted to existing Planmeca EC and CC Proline models. This makes the adoption of digital technology more affordable and more attractive to those dentists who already have panoramic machines from Planmeca.
Trophy Radiology, Inc., (now Trextrophy) also makes a panoramic CCD system, called the DigiPan PC kit for adaptation to the Instrumentarium machine, the OP 100. They suggest a 360dpi laser printer for radiological imaging. Both of these digital panoramic systems require a computer workstation with minimum requirements of 166 MHz, 32 MB of RAM, and a hard drive with 2 to 4 GB of memory.
Why will dentists adopt CCD technology faster than Intraoral digital imaging?
The answer is because unlike intraoral devices, there is no wire. Panoramic radiography does not require that the sensor be placed in the mouth. There is no difference in positioning technique or image acquisition from conventional panoramic imaging. The second reason is the image itself. The resolution of the digital images is already equal to that of standard panoramic films. CCD images have slightly less line pair resolution than film. This is not the case with the panoramic images. And, there still are all the advantages of CCD imaging; namely,
| Consistent quality; | |
| Elimination of the darkroom; | |
| Improved disease detection; | |
| Electronic image processing; | |
| Instant image viewing; | |
| Greater exposure latitude; | |
| Remote consultation; | |
| Reduced X-ray exposure; | |
| Elimination of hazardous chemicals; and | |
| Improved patient education and care. |
Cost
The initial cost may be discouraging to some dentists. Because the technology is so advanced and new, the cost of a new CCD based panoramic machine will be from $40,000 to $50,000. However, it is probable that the dentist will keep the X-ray machine for 10 to 20 years, which would be plenty of time to recoup the investment and profit from the use.
Training
Most dentists and dental auxiliaries have not had formal training in panoramic radiographic technique. The original panoramic technology was developed and marketed long before the education caught up. This has left many dentists with the opinion that panoramic images are inferior. This is not the case. Unfortunately, the sales representatives that installed the devices in doctors' offices were themselves not trained in panoramic positioning techniques. Even today, many radiologists are still asked to give one-day programs on panoramic techniques to study clubs, district dental societies, and national meetings. The fact that there is no difference in the positioning technique between conventional and digital panoramic radiography will not guarantee that a dentist will automatically have better images. Errors will still be made until the dentist and staff receive proper training. Fortunately, there are journal articles, videotapes, lectures at meetings, and well trained company representatives to help remedy this problem. Soon there will even be CDROMs containing radiology training, including advanced techniques like panoramic imaging.
Computer Literacy
Training in panoramic technique is not the only educational issue. Just as with intraoral digital radiography, dentists and their staff must be able to master the image processing techniques the electronic type before they will feel comfortable with digital imaging of any kind. Manufacturers are aware of this and are developing image processing programs that are user-friendly. Most of the operations will be menu and/or icon based and easy to master quickly. The perceived problem of "technoilliteracy" will not be a major problem for most dentists as new training programs are developed by companies to fill this void in dentist consumer education.
It is conceivable that, with two passes (exposures), software provided with the digital panoramic machines will be able to provide three-dimensional information and display, just like computed tomography in medicine. This is only possible because of the very low X-ray exposure required by CCD detectors for image acquisition. By making a second "pass" after changing the vertical angulation slightly, the software program might have the numerical information required to "reconstruct" a 3-D image. This would then allow a dentist to visualize the bony defect architecture on the monitor image, rather than having to infer it from the two-dimensional radiographic images and clinical probing depths. The image could be rotated and viewed from different directions to assist the diagnosis. Dr. Richard Webber has recently developed program software to render "tomosynthetic" images slices through a contact point, for example that allow the clinician to "step through" the interproximal surface of a tooth 0.5 mm at a time from buccal to lingual. This is very powerful as a diagnostic and patient educational tool.
Digital imaging is here to stay. Both intraoral and panoramic digital imaging based on CCD systems or reusable storage phosphors require computer workstations and program software for image display, diagnosis, and patient education. Those practitioners who own computers are on their way to the future in digital imaging. It is only a matter of adopting the systems, acquiring some minimal additional training, and using the technology with all its advantages. There is little reason to put off the decision to go digital.
Authors
Dale A. Miles, DDS, MS, is a professor and chair of the Department of Oral Health Science at the University of Kentucky College of Dentistry.
Robert P. Langlais, DDS, MS, is a professor in the Department of Dental Diagnostic Science at the University of Texas Health Science Center at San Antonio.
Edwin T. Parks, DMD, MS, is in the Department of Oral Surgery, Medicine and Pathology at Indiana University School of Dentistry.
References
![]() Previous Chapter
(Chapter 1)
Previous Chapter
(Chapter 1)
![]() Next Chapter
(Chapter 3)
Next Chapter
(Chapter 3)