| Contents | Previous | Next |
Clinical supervisors in today's global workplace are faced with the responsibility of assuming a broad range of roles and tasks. New clinical supervisors often feel like they are blindly running a maze.
The frequently encountered switchbacks, blind alleys, doors opening into brick walls and dead-ends create frustration, annoyance and stress. Without the proper skills, it is nearly impossible for supervisors to navigate confidently and competently through the variety of required roles and responsibilities that are thrust upon them daily.
Clinical supervision has been defined in several ways throughout the literature. Here are some examples:
An intervention that is provided by a senior member of a profession to a junior member or members of that same profession. This relationship is evaluative, extends over time, and has the same simultaneous purposes of enhancing the professional functioning of the junior member(s), monitoring the quality of professional services offered to the clients she, he or they see(s), and serving as a gatekeeper for those who are to enter the particular profession (Bernard & Goodyear, 1992, p.4).
An experienced therapist safeguarding the welfare of clients by monitoring a less experienced therapist's competence with clients in a clinical setting with the intent to change the therapist's behavior to resemble that of an experienced family therapist (Mead, 1990, p.4).
Clinical supervision is the construction of individualized learning plans for supervisees working with clients (Liddick, 1994, p. 1).
Clinical supervision is defined here as a dynamic, genuine, authentic and aligned interrelationship that exists among the clinical supervisor, the supervisee and the client. Primary elements of this interrelationship include competency-based coaching, mentoring, teaching, assessment, evaluation, competence feedback and accountability. The clinical supervisor continuously safeguards the client's well-being, while simultaneously enhancing the supervisee's incremental professional skills development and ongoing learning.
By looking down over the entire journey with a bird's eye view, nine navigational skills related to the clinical supervision process come clearly into focus.
|
When used consistently, these skills can make your daily "run" through the maze less frustrating and more enjoyable.
All of these skills are anchored in the context of relationship. The supervisor's central role is to create and sustain collaborative working relationships with each supervisee and client. In your daily activities, you must strive to create and nurture an environment of respect, trust, openness, honesty and dependability with every supervisee and client within your practice. The foundation of effective global workforce clinical supervision and practice management is creating an inclusive environment.
Consider the dynamics between the staff members of this Family Service Center.
Henry has been an employee at the Family Service Center for seven years. He has worked with a variety of families struggling with a wide range of relationship issues. He was recently promoted to clinical supervisor of the internship program.
Kathryn, the clinical director, has called Henry into her office this Monday morning, to discuss his new position and responsibilities. She says,
"Henry, it's my pleasure to welcome you to our management team here in the Family Service Center. You've been a strong team player and a significant contributor to the success of our department over the past several years."
"Kathryn, thanks a lot. I can't tell you how anxious I am to get started. I've been waiting for an opportunity to advance for awhile now and I'm really grateful you've given me this chance."
"You're welcome, Henry. I know you've been applying for a promotion whenever they've been posted, and I think you’re the best match for this position. I'll get you registered for our upcoming leadership and clinical supervisory skills training program next month."
"Well, I don't think it's really necessary for me to take that training class, Kathryn; after all I've been doing the work for over five years now. The main things are job knowledge and experience and I have both under my belt."
"Henry, you do know the job and you've definitely got the experience but there is more to being an effective leader and clinical supervisor than those two things. There are several skills that are essential for success in your new role."
"That may be true for some people, Kathryn, but I've been around long enough and seen enough that I know what it takes. What the Family Service Center needs most is for a supervisor to take action and make things happen, not form committees and generate more paperwork!"
"Okay Henry, I may regret it later, but let's try it and see what you can do!"
Later, Monday afternoon, Henry is meeting with his new internship group for an orientation session. Henry approaches Carl to welcome him to the meeting.
"Carl, I was really excited to see your name on the intern roster and to have you on my team. You may not realize it, but we're both graduates of the same university! Yes, Stanford! You know, Stanford was tough but I figure if you can get through that program you can be a success anywhere."
"Hey, I didn't know that. When did you graduate, Henry?"
"I was just two years ahead of you, Carl!
“Carl, I'm going to need a peer team leader. It's really a huge responsibility and there will be a lot of high visibility. If you do well, it will be career enhancing for both of us. Why don't you think about whether or not you'd like to take on that role and get back to me, okay?"
"Thanks, Henry, I'll do that."
"Carl, I have a copy of the intern program guidelines and I'd really appreciate it if you'd look it over and make any recommendations you think might be helpful for the program. Do you think we could get together by Wednesday to discuss it?"
"Sure, no problem, Henry. I'll go over it and let you know what I think. What time do you want to meet on Wednesday?"
"Well, I'm meeting with Paul, our center's president, for lunch, after that I will have some time about 2:00 pm. Now that I think of it, are you free for lunch? It would be a perfect opportunity for me to introduce you to Paul if you haven't already met."
"As a matter of fact, I am free, and no, I haven't met Paul yet. Thanks for thinking about me, Henry."
"No problem, oh, by the way, you do play golf don't you? Oh, and before I leave, let me give you my numbers. Here are my cell phone, pager and home numbers. Call me anytime, okay? See you Wednesday about 11:30 am.”
Next, Henry goes up to Juanita and says,
" Hello, Joanne, how are you this afternoon?"
She says,
"I'm fine, Henry, and please call me, Juanita. How are you?"
"Oh, Juhnita…. er.… Juneta,… uh, I mean… Juanita,… I'm sorry, I'll try to get it right from now on. I'm great. Anyway, I see you've joined the Family Service Center after being in Child Protective Services for several years. I guess you must have finally gotten fed up with all the red tape in a government agency, huh."
"Actually, Henry, I applied for this opportunity because of the skills and training I received at CPS. I have a lot of experience in family work and I'm hoping to have new opportunities to apply my skills as well as develop new ones with some family cases here at the Family Service Center."
"Really, I didn't realize that. My strengths are in family treatment too, so I was thinking of having you assist Susan and Bill with the intake process. If you need any help or have any concerns be sure and speak up, both Susan and Bill have a lot of expertise in that area."
"Okay Henry, but I was really hoping to be more involved in the family treatment side too. Do you think I could play a part in that area as well?"
"Look, Juanita, I think it would be best for the team and for the clients if you just started slow and easy with the intake role. You'll have a lot of help and the pressures won't be as severe. You can handle some pressure and tight deadlines, can't you?"
You will be revisiting Henry and his colleagues from time to time as you move through each chapter. Keep this scenario at the Family Service Center in mind as you take a closer look at Skill #1.
Practicing clear communication is the first skill that clinical supervisors must develop to effectively practice global workforce clinical supervision and practice management. The communication process includes four primary elements. A Sender has a Message to convey to a Receiver and the Receiver gives Feedback to the Sender in response to the Sender’s Message. The Communication Model below diagrams this process.
During your reflection on the model, I imagine it became clear that more was going on between the Senders and Receivers in a conversation than the simple, clear exchange of messages and feedback. If you could clearly express yourself every time you send a message and have it received in the way you intended it by the other party, you would have relationships free of most unnecessary conflicts, at least those resulting from misunderstandings between communicators.
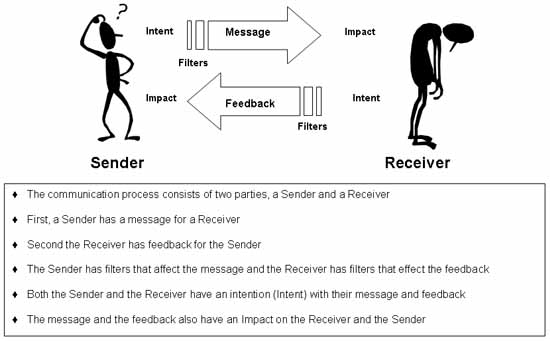
The communication process is much more complicated than the diagram above with a sender, receiver, message and feedback. It also includes the components of filters, intentions and impacts. Each sender and receiver has a set of filters, and specific intentions around their messages. Each party is impacted by the message sent and the feedback given as well as each party’s perceived intentions throughout the conversation. These components are added to the model later in this chapter.
We each have a set of filters that affect how we view the world. Sociologists sometimes refer to this concept as worldview. Our filters are a composite of our unique life experiences. Each of us has a unique set because no two human beings are exactly alike in every aspect of their humanity.
Loden and Rosener (1991) created the concept of dimensions of diversity. They defined six primary dimensions that serve as independent core elements that are unchangeable. They are age, ethnicity, gender, physical abilities/qualities, race and sexual/affectional orientation. They also defined eight secondary dimensions that are changeable. They are educational background, geographic location, income, marital status, military experience, parental status, religious beliefs and work experience.
I have adapted their concept of diversity dimensions to create the Diversity Spheres Model to illustrate the concept of filters and worldview. The diagram appears on the following page.
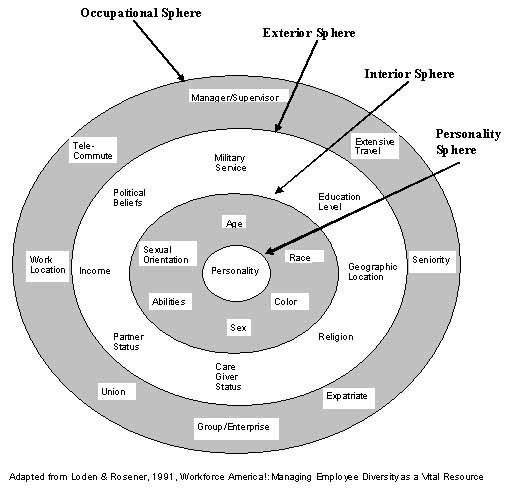
The Diversity Spheres diagram graphically illustrates four general spheres with several specific characteristics within each dimension that collectively define our personal diversity filters. The dimensions within each sphere may influence one another. The spheres themselves may also influence one another from the core moving outward. The various dimensions within and between the spheres are intrinsically interwoven creating a unique tapestry of our human experiences. This collective interaction defines our worldview or our unique, personal diversity filters.
The innermost sphere is Personality. Your personality is formed during childhood and it affects all aspects of your life experience.
There are numerous theories of personality and its origins, but most are traceable to Hippocrate‘s ancient theory of the four quadrants of personality. These were originally labeled Choleric, Sanguine, Phlegmatic and Melancholy. Many modern theorists have re-named these quadrants but the traits remain the same.
The most widely accepted contemporary theory of personality is frequently referred to as The Big Five Theory or the Five Factor Model. This theory suggests that there are five dimensions (factors) of personality traits. These are:
|
Factor
Negative Emotionality Extraversion Openness Agreeableness Conscientiousness |
Anchors for Two Extremes
Resilient v Reactive Introvert v Extravert Preserver v Explorer Challenger v Adapter Flexible v Focused |
The combination of traits making up our unique personalities contributes to part of our uniqueness. Many people have similar personalities, but our individual life experiences combined with our personalities make us truly unique human beings. Our personalities infiltrate all other aspects of our being. These traits affect each of the diversity spheres much like looking through a prism affects light and color or how three-dimensional glasses affect our perceptions when watching a 3-D movie projection.
The second sphere of our diversity filters is called Interior. These are things intrinsic to whom we are, internal elements of our humanity that we have little or no control over changing or altering in our life experiences. The dimensions: age, race, color and sex (gender) are determined genetically and biologically. Abilities can be limited by congenital defects and they can also be impaired by serious illness or injury later in life.
Sexual orientation is a heavily debated issue in the scientific and theological communities. The scientific community has produced scholarly research and findings supporting two opposing views; one view is the position that sexual orientation is genetic, biological or environmental and second is the position that individuals have the ability to both choose and change their sexual orientation. The theological community has the same split. Religious scholars and theologians have written extensively about both positions. Consider this Gallup Poll News Service release:
A new study, authored by Dr. Robert L. Spitzer of Columbia University and scheduled to be presented at a meeting of the American Psychiatric Association, is furthering the already intense debate on the cause of a person's sexual orientation. The findings of the study imply that a homosexual can choose to become straight if he or she wants to. Other scholars who criticize the legitimacy of "reparative therapy" are contesting the findings of the study. The average American appears to be as divided on the issues as are those who study it. Gallup has asked the public for a quarter of a century, "In your view, is homosexuality something a person is born with or is homosexuality due to other factors such as upbringing or environment?"
In Gallup's latest poll on the topic, conducted February 8-9, 1999, 34% of the public believes homosexuality is something a person is born with, 44% believes it is caused by environment and upbringing, while another 13% volunteer that it is a combination of both. Belief that homosexuality is a trait a human is born with has increased since the 1970s and 80s. In 1982, 17% believed it was something a person was born with, while 52% believed it was due to upbringing and environment. In 1977, just 13% thought homosexuality was genetic.
The majority of Americans (83%) believe that homosexuals should have equal rights when it comes to job opportunities. However, the public is split on whether homosexuality is an acceptable lifestyle and whether homosexual relations should be legal. Currently, 50% of Americans think homosexual relations between consenting adults should be legal, while 43% say they should not. This trend has remained relatively constant since Gallup began asking it in 1977. Regarding acceptance, 50% of Americans currently say they believe homosexuality is an acceptable lifestyle, while 46% say it is not. The public's acceptance of the homosexual lifestyle has increased significantly since Gallup began asking the question in 1982. At that time, 34% thought it was an acceptable lifestyle (Carlson, 2001).
Despite the controversy of whether or not it’s a choice, sexual orientation is a very real and important dimension of diversity. It influences our perception of the world and of others, and it influences the treatment we receive from one another depending on how we identify ourselves.
The third sphere is called Exterior. These are things outside ourselves over which we can sometimes exercise choice or options. Some of us have experienced more frequency or variety than others in these dimensions. Each of these dimensions, military service, education level, geographic location, religion, care giver status, partner status, income and political beliefs are all determined by factors external to our beings. Sometimes we may believe that our choices are severely limited because of the consequences we may endure by choosing change in one of these dimensions. At other times, earlier choices may have limited our future choices in these dimensions.
When we choose to limit our education level, it may sometimes limit our income opportunities. When we choose caregiver status, parental or guardian, we may limit our opportunities in terms of geographic location, partner status, or income opportunities. If you are in military service you may lose the ability at times to choose your geographic location or you may experience multiple relocations throughout the course of your tours of duty. Certain religious practices may influence your choices politically. Additionally, these choices may influence those in our care, dependent children or adults. This impacts their worldview and diversity filters too.
The fourth sphere is called Occupational. These are the various roles, relationships, and experiences you may encounter throughout your work life within an organization. These dimensions include: manager/supervisor role, extensive business-related travel, seniority, expatriate status, working in a specific group or enterprise, union affiliation, specific work locations (corporate, remote or satellite office), and telecommuting (virtual office).
If you work for a large company, or for the same company for many years, you may have more opportunities to experience a wider variety of these dimensions. If you work for a variety of employers in different fields, you may also have a broader experience range within the occupational sphere dimensions.
Whenever you communicate a message to someone else, you have an intention in mind. You intend to get a response by impacting the receiver in some way. Your intentions may be conscious, unconscious, or both depending on the circumstances surrounding the conversation.
A sender's message always impacts the receiver. When the receiver gives feedback to the sender, there is an intention behind that message and an impact on the receiver too. This cycle continues throughout the conversation.
Look at the Communications and Filters Model on the next page. It illustrates how intent, impact and filters make the communications process much more complex.
Going back to the Family Service Center vignette, when Kathyrn, Henry, Carl and Juanita were talking with one another, you can find several examples of intent and impact. First, consider this interaction between Kathryn and Henry:
[Kathryn speaking] "You're welcome, Henry. I know you've been applying for a promotion whenever they've been posted, and I think you’re the best match for this position. I'll get you registered for our upcoming leadership and clinical supervisory skills training program next month."
"Well, I don't think it's really necessary for me to take that training class, Kathryn, after all I've been doing the work for over five years now. The main things are job knowledge and experience and I have both under my belt."
"Henry, you do know the job and you've definitely got the experience but there is more to being an effective leader and clinical supervisor than those two things. There are several skills that are essential for success in your new role."
Kathryn's intent was to acknowledge Henry's skills and experience and to let him know that he needed new skills and training for a new role as a supervisor. The impact on Henry was a perception that Kathryn didn't understand his abilities and she wasn't giving him credit for his past track record.
Henry's intent was to help Kathryn understand that he believed job knowledge and experience were the essential tools for successful supervision. Kathyrn's intent was to validate Henry's ability and emphasize his need for additional skills training, but she did not give specific examples. Kathryn also failed to follow through with her intention to enroll him in the upcoming training.
Next, consider this interaction between Henry and Juanita:
"Okay Henry, but I was really hoping to be more involved in the family treatment side too. Do you think I could play a part in that area as well?"
"Look, Juanita, I think it would be best for the team and for the clients if you just started slow and easy with the intake role. You'll have a lot of help and the pressures won't be as severe. You can handle some pressure and tight deadlines can't you?"
Juanita's intention was to clarify with Henry that she was hoping to be more involved with family treatment because of her experience and skill in this area. The impact on Henry was that she didn't know her own limitations and weaknesses and could easily over-extend herself by taking on too much too soon.
Henry's intent could have been to "protect" Juanita from overextending herself and getting in "over her head," because of his belief that she would need "a lot of help" and less pressure. He also seemed concerned about her ability to handle "tight deadlines." The impact on Juanita was that Henry didn't believe she had the capability to do the job.
In the expanded communications model that follows, you can see how filters influence both the intent of the message from the Sender to the Receiver and the feedback message from the Receiver to the Sender. Filters can have a complex impact on both the Sender and the Receiver when several filters are influencing the message and feedback cycle.
Most of us didn't learn to listen until we began our graduate training in counseling or psychology. We had previously learned to talk "at one another" instead of how to hear one another. We practiced using the time when someone else was speaking to us to think about our own response or feedback that we wanted to give when they quit speaking. The result was often two people talking at one another, making assumptions, drawing conclusions and second-guessing one another in a frequently futile attempt to communicate clearly.
When two people have strong feelings about a topic and they are eager to talk with one another, they can easily fall into a pattern of talking at one another. They each try to "listen" to the other person, but the focus is usually on wanting to be understood, accepted, agreed with or supported in some way. If one person is fearful of losing what they are seeking, they may tend to interrupt, challenge or confront the other person. Sometimes, they will impatiently assume they know what the other person is thinking or feeling at the moment. This frequently appears in the form of finishing a sentence or thought, or suggesting a word or phrase for the other person.
Active listening is a process of attending to the speaker in a conversation as an active listener. It includes noticing the content, meaning and context of the speaker's message and suspending our own thoughts, agenda or contributions until you have a clear understanding of the message being shared.
Several steps are required to competently perform this skill. First, the listener needs to focus his or her attention directly upon the speaker. This can be accomplished by maintaining frequent eye contact, mirroring the speaker's posture, tone and volume and waiting until you are sure the speaker has finished expressing his or her thoughts before responding with feedback.
Second, it is important to suspend the temptation to become preoccupied with your own thoughts, responses, ideas or opinions while the other person is speaking. You can easily accomplish this by periodically paraphrasing what you are hearing, and ask for clarification from the speaker. For example,
"What I'm hearing you say is that if I listen to understand, instead of listening to get a chance to speak, I may have more effective conversations. Is that what you mean?"
If the speaker thinks he or she has been misunderstood, the speaker now has an opportunity to clarify the message or meaning. By listening and reflecting or paraphrasing what you have heard, you are better able to focus your attention on the speaker.
If you are able to actively engage the speaker with active listening skills, you will have a much better chance of clearly understanding the message. Fourth, once you have clarity of understanding, you can begin to give focused feedback, including your personal thoughts and opinions, in response to what you have clearly heard and understood.
You communicate much more nonverbally than you do verbally during a conversation. Developing skills in attending to the nonverbal messages being communicated is essential if you want to better understand other people's messages and intentions.
Attending to the speaker's body language is an important part of active listening. Noticing the speaker's posture, gestures, nods and placement of arms, legs, hands and feet during a conversation will provide cues for interpreting meaning in the message.
Noticing congruence or incongruence between body language and verbal tone, speech inflection and content helps the listener interpret meaning from the speaker's message. If the speaker is talking about painful, sad or fearful experiences and the speaker is smiling or laughing while sharing, or conversely, if the speaker is crying, trembling or murmuring while speaking of happy, carefree or enjoyable experiences the affect is incongruent with the message.
Now let's revisit the concept of filters and explore in depth how filters influence your intentions when you send and receive messages and how the messages you receive as feedback from someone else impact you. Earlier, you explored the Diversity Spheres Model and the various dimensions of diversity within each sphere. Turn back to the Diversity Spheres Model for reference as you complete this exercise.
Identify twelve specific characteristics that describe a specific aspect of who you are as a unique individual. Choose three from each Sphere in the model, Personality, Interior, Exterior and Occupational and record them below. For example:
Personality: introverted, extroverted, impulsive, controlled, intuitive, practical
Interior: 35 years old, Hispanic, Female, Heterosexual
Exterior: Republican, retired Air Force Captain, Married
Occupational: Clinical Supervisor, Non-union, 3 satellite offices
Personality Sphere
Interior Sphere
Exterior Sphere
Occupational Sphere
Review the specific diversity aspects you have listed above and prioritize them from 1 to 12. Use a ranking of 1 to represent the aspect that most influences your interactions and decision-making with others. Use a ranking of 12 to represent the aspect that least influences your interactions and decision-making with others.
Describe how your top three diversity aspects influence your interactions with coworkers, supervisees and clients.
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
Describe how your top three diversity aspects influence your decision-making in interactions with coworkers, supervisees and clients.
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
What did you learn from the Personal Filters Exercise?
How can you apply your learning to your clinical supervision practice?