| Contents | Previous | Next |
Two major questions are examined in this chapter. First, how does panic disorder affect the course of chronic medical disorders afflicting the patient? Second, does panic disorder predispose the patient to specific medical disorders?
As discussed in chapter 9, scientists have hypothesized that panic disorder results from central dyscontrol of the brain alarm system that warns the patient about external dangers. The locus ceruleus, a cluster of noradrenergic neurons located in the pons, may be the central control mechanism for the autonomic nervous system (Redmond 1979). Activation of the locus ceruleus has been associated with fear and alarm reactions in primates (Redmond et al. 1976). Moreover, bilateral lesions of the locus ceruleus in animals lead to failure to show normal cardioaccelerator responses (increased pulse and blood pressure) to threatening stimuli (Snyder et al. 1977).
The locus ceruleus has projections to many regions of the brain associated with responses to fear and pain. It also has projections to the cerebral cortex which, as Svensson (1987) emphasized, might be involved with the interpretation of "meaning" or relevance of a stimulus to the individual. Finally, the locus ceruleus has projections to limbic areas, such as the amygdala, which are important regions for emotional and cardiovascular control.
Activation of the locus ceruleus appears critical to the defense reaction that mobilizes an individual for the "fight or flight" response (Svensson 1987). This reaction involves increased vigilance and fear, neurogenic activity of sympathetic fibers to the heart, splanchnic region, and kidneys, central suppression of vagal restraint of the heart, and an ensuing blood pressure elevation mainly caused by increased cardiac output. The sympathetic activation of the kidneys is associated with increased rennin release and activation of the reninaldosterone axis as well as mobilization of glucocorticoids.
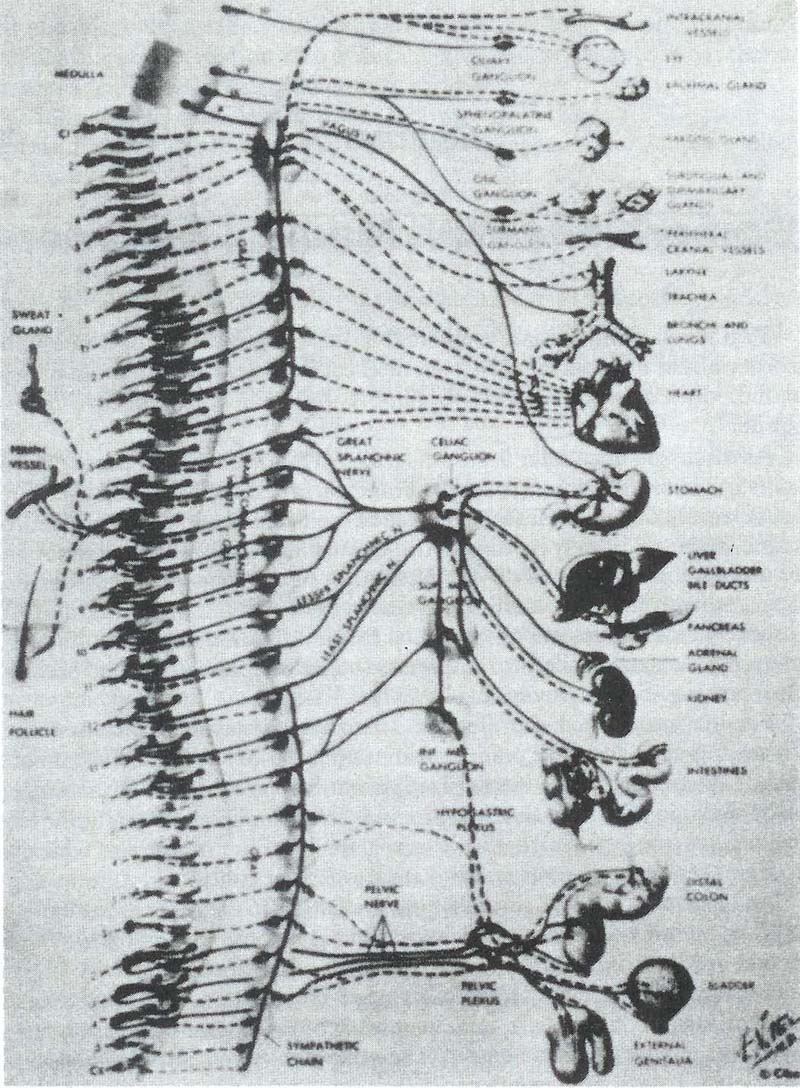
Figure 3 depicts the multiple connections between the autonomic nervous system and the peripheral organ systems. Panic disorder may be caused by dyregulation of the locus ceruleus causing the initiation of fight-or-flight reactions at inappropriate times, i.e., when there is no symbolic or actual danger (Charney et al. 1984). When panic disorder or major depression is associated with chronic medical illness, the psychiatric illness causes amplification of symptomatic complaints of the medical illness, such as increased reports of angina in the patient with chronic angina pectoris and panic disorder (Bridges and Goldberg 1985). This worsening of symptoms is probably secondary to both the increased tendency to report symptoms and a worsening of physiologic illness secondary to sympathetic nervous system arousal. For example, in a patient with angina pectoris and severe coronary artery disease, the increased sympathetic arousal accompanying a panic attack could cause increased heart rate, blood pressure, and cardiac output, potentially precipitating a bout of angina pectoris. These patients may present with increased chest pain after being controlled in the past on cardiac medications such as beta-blockers, nitrates, or calcium channel blockers. A vicious cycle of symptoms may ensue, with panic attacks provoking angina and anginal episodes provoking panic. In these cases, once the panic disorder is effectively treated, the chest pain episodes may decrease.
| Figure 3. Autonomic nervous system |
|
|
| Source: The CIBA Collection of Medical Illustrations, by Frank H. Netter, M.D. Volume I, Plate 54. Copyright 1962 by CIBA-GEIGY Corporation. Reproduced with permission. All rights reserved. |
Panic Disorder with Angina PectorisA 60-year-bld male treated with propranolol for angina pectoris began to visit his physician with increased frequency due to worsening angina. Calcim channel blockers and long-acting nitrates were prescribed, but they did not decrease the anginal episodes. Prior to referring the patient for repeat angiography, psychiatric consultation was obtained because the patient had had a marked increase in nervousness and anxiety. The patient revealed severe financial problems necessitating filing for bankruptcy and problem with the recent divorce of his daughter. Acute episodes of shortness of breath, chest tightness, dyspnea, tremulousness, and dizziness had been occurring for the last 2 months, often preceding more typical episodes of substernal chest pain radiating into his left arm. He had become increasingly afraid to go out unaccompanied by his wife because of these episodes, and he had become progressively more isolated socially because the episodes seemed to occur more often when in groups or crowds of people. He was diagnosed as haying panic disorder and started on imipramine, 25 mg per day, increasing by 25mg every 3 days. On a total dosage of 75 mg his angina was once again well controlled on his original regime. He remained well over a 1-year period. |
Noyes and colleagues (1980) addressed the association of panic disorder with specific medical illnesses by following patients with panic disorder and a surgical outpatient control group over a 6-year period, comparing the incidence of six illnesses thought to have a psychophysiologic basis. Patients with panic disorder were found to have a significantly higher rate of hypertension and peptic ulcer disease over this period. Katon (1984) also found that 55 primary care patients with panic disorder had a significantly higher rate of peptic ulcer disease (diagnosed by endoscopy) and hypertension than did clinic controls. In a second epidemiologic study of panic disorder in primary care, Katon (1986) found that 13.6 percent of primary care patients with panic disorder had hypertension versus 4.4 percent of controls (p = .03) but did not find a higher prevalence of peptic ulcer disease.
Clinically, patients often have labile hypertension during active panic attacks, but once these attacks are blocked by psychopharmacologic agents, the labile hypertension usually subsides (Balon et al. 1988; Freedman et al. 1985; Shear 1986). The possibility that panic disorder may be causal in the development of hypertension is further suggested by the fact that 17 of 22 patients in the Noyes et al. (1980) study developed hypertension 2 or more years after they developed panic disorder. An intriguing biologic finding also supports this hypothesis. Several research groups have found significantly higher resting levels of epinephrine in arteriolized venous blood in patients with panic disorder versus controls (Villacres et al. 1987; Nesse et al. 1984; Appleby et al. 1981). A subset of hypertensives had higher epinephrine levels than controls, and chronically high epinephrine levels may lead to chronic peripheral vasoconstriction over time (Weder and Julius 1985).
Studies of patients with panic disorder referred to psychopharmacologic trials in anxiety disorder clinics found no increase in hypertension in these patients, so the above findings may be specific to patients with panic disorder who frequently visit primary care physicians. Future research questions that need to be addressed include: Is there a subgroup of patients with panic disorder who have labile hypertension initially as a result of hyperactive central noradrenergic mechanisms involving the locus ceruleus who are not adequately treated and then develop chronic hypertension? Does the labile hypertension, locus ceruleus, and sympathetic nervous system hyperactivity and high peripheral epinephrine levels cause long-term irreversible peripheral vasoconstriction leading to chronic hypertension in these patients?
Panic Disorder Associated With Labile HypertensionMrs. S was a 28-year-old laborer and fishing guide who presented with an acute episode of chest pain, tachycardia, “head rushes”, and labile hypertension. His blood pressure often went up as high as 200/115 with these episodes. Over a 6-month period, he was hospitalized three times for these symptoms. Cardiac enzymes, treadmill test, and echocardiogram revealed only mitral valve prolapse. He was started on atenollol 50mg twice a day, but this did not relieve his symptoms. He was referred to an endocrinologist for the acute episodes of chest pain and labile hypertension. Separate workups for pheochromocytoma, carcinoid, and thyroid disease were negative. Over the 6-months period, he lost his job and had to apply for welfare and ran up $10,000 in medical bills. He was finally referred for psychiatric consultation where he revealed that the acute episodes of chest pain were accompanied by rapid heart beat, sweatiness, dizziness, shortness of breath, tingling in hands and feet, and a sense of impending doom. He also suffered from irritability, insomnia, anorexia, 40-pund weight loss, and lack of pleasure in his usual activities. He was diagnosed as meeting criteria for panic disorder and major depression and was started on imipramine, 50 mg daily increasing to 250 mg, and he rapidly recovered over a 1-month period. He started back to work in a lumber mill and worked steadily for the succeeding year. His labile hypertension resolved completely, and he was able to taper and discontinue his atenolol over a 1-month period. |
Existing studies of associations between panic disorder and cardiovascular orbidity and mortality are all retrospective. In two independent studies, oryell and colleagues (1982,1986) found an increased mortality for male panic disorder patients, the increase being accounted for by cardiovascular death and suicide. These results were based on small numbers of expected and observed saths. In the first study, six men were expected to die and 12 men died; in the second, 1.8 total male deaths were expected and four men actually died, three am cardiovascular causes. In three other studies of "neurotic patients," some whom had panic disorder, no link between neurotic illness and cardiovascular morbidity was found (Martin et al. 1985; Black et al. 1985; Winokur and Black 87).
One last study associating panic disorder with cardiovascular morbidity (Kahn et al. 1987) reported that patients with idiopathic cardiomyopathy had an increased prevalence of panic disorder (51 percent definite panic disorder, percent probable panic disorder) compared to cardiac patients with post infarction cardiac failure (5.5 percent definite and 17 percent probable panic disorder) and patients with rheumatic or congenital heart disease (0 percent definite or probable panic disorder). All patients were awaiting transplants, and most patients, the panic disorder preceded the symptoms of idiopathic rdiomyopathy. The authors noted that both ectopic atrial tachyarrhythmias (Gillette et al. 1985) and catecholamine-secreting pheochromocytomas (Van liet et al. 1966) can cause myocarditis and cardiomyopathy and hypothesized at either autonomically induced small-vessel changes or high catecholamine levels that may be associated with panic disorder could lead similarly to myocartis and progressive cardiomyopathy in some patients with panic disorder (Kahn et al. 1987). Clearly, this study needs to be replicated, but the results are intriguing.
MVP refers to a condition in which the leaflets of the mitral valve are redundant and sag toward the left atrial chamber during ventricular systole (Dager et al. 1986). This sagging, with sudden tensing of the submitral apparatus, results in auscultatory findings of one or more systolic clicks and the presence of a mid-to-late systolic murmur of mitral regurgitation (Devereux et al. 1976). Maneuvers that decrease left ventricular volume (such as abrupt standing or inhalation of amyl nitrate vapors) increase leaflet redundancy and may unmask occult MVP. Clinical symptoms of MVP include atypical chest pain, dyspnea, tachycardia, palpitations, light-headedness, syncope, fatigue, and anxiety (Barlow et al. 1968; Devereux et al. 1976). Reported complications included sudden death, progressive mitral regurgitation, and bacterial endocarditis (Wynne 1986). These signs and symptoms and their complications have been called the MVP syndrome (Devereux et al. 1976).
MVP is a controversial syndrome with highly variable prevalence rates reported in the general population, conflicting studies reporting prevalence of complications and autonomic defects, and various criteria used to define the "disease" (Wynne 1986; Margraf et al. 1988). Thus, reported prevalence rates have ranged between 5 and 21 percent. Much of this variability is due to the different criteria used for diagnosis. As Dager and colleagues (1986) emphasized, the diagnosis of MVP still has no "gold standard." The changes in mitral valve mobility are in reality continuous, not dichotomous variables (Wynne 1986). The continuum of changes includes on the one end a near "flail" leaflet and florid mitral regurgitation and on the other equivocal, nonspecific thickening with minor abnormalities of valve closure and no corroborative physical findings. The former severe abnormality may be associated with connective tissue disorders such as Marfan's or Ehlers-Danlos syndromes (Wynne 1986).
Different studies of prevalence have used different criteria for diagnosis. In one study, the prevalence dropped from 13 to 0.5 percent when more stringent criteria were employed (Warth et al. 1985). Most of the older studies used M-mode echocardiography, which maybe subject to serious methodologic errors leading to false positive and negative findings (Dager et al. 1986; Margraf et al. 1988). The more recent 2-D echocardiographic studies provide a cross-sectional representation of cardiac structure and valve leaflet anatomy and is considered a much more accurate test. However, there is still no consensus among cardiologists regarding the minimum extent of mitral valve leaflet sagging required to make the diagnosis, especially in the absence of the corroborative physical findings. Thus, while echocardiography is considered a more sensitive test to detect MVP than is auscultation, there is also great variability in the criteria to detect MVP as well as the application of these criteria (Wynne 1986; Dager et al. 1986; Margrafet al. 1988). Recent estimates of the retest and interrater reliability of raters from the same laboratory using the same criteria have demonstrated a lack of diagnostic precision (Margraff et al. 1988; Dager et al. 1986). Reliability from raters from different institutions is even less. Thus, German and colleagues (1986b) demonstrated that in a series of 15 patients with panic disorder, one rater diagnosed MVP in 9 patients while a second did not make the diagnosis in a single patient.
A recent editorial by Wynne (1986) suggested that two groups of subjects carry the diagnosis of MVP. The first consists of persons in whom .the disorder is principally an echocardiographic finding. These people are no more symptomatic than controls, have no more arrhythmias, and are often free of the typical auscultory findings and have a low risk of complications. The echocardiographic findings in this group are probably normal variants and reflect the technologic advances in defining valve motion, while emphasizing the difficulty in differentiating variants of normal valve mobility. The second group consists of patients who typically not only have evidence of prolapse on echocardiography but who also have clinical findings of mitral valve regurgitation (with or without a systolic click). These people may have symptoms related to valvular insufficiency and appear to have an increased risk of infective endocarditis as well as progressive mitral regurgitation. Two useful markers have been identified to help differentiate between the first group (with trivial MVP) and the second group (with important MVP): (1) the degree of redundancy of the valve, a finding that can be defined echocardiographically and (2) the presence of mitral regurgitation on physical examination (Wynne 1986). Thus, Nishimura and colleagues (1985) recently found that almost every patient with a complication of MVP had redundant valves as indicated by an increase in mitral valve leaflet thickness of 5 mm or more. Even in this group, the complications of endocarditis or cerebral embolism averaged less than 1 percent per year. These complications tend to occur in older patients and in males.
Do patients with mitral valve prolapse have higher rates of panic disorder? Margraf and colleagues (1988) recently reviewed the eight studies in the world's literature that asked this question and reported no elevated prevalence of panic disorder in MVP patients compared to subjects with other cardiac complaints. However, both patients with MVP and control patients in a cardiac practice had a higher prevalence of panic attacks than did controls with MVP who were not seeking medical help. These data suggest that patients with MVP and panic are most likely to seek medical help, probably secondary to the symptoms caused by severe anxiety.
Margraff and colleagues (1988) also reviewed the world's literature on MVP in patients with panic disorder. They pointed out the many methodologic problems in these studies including lack of control groups in all but five studies, lack of blinded raters for the psychiatric diagnosis, and lack of homogeneous samples (some included depressive or generalized anxiety disorder patients). Eighteen percent of the patients with panic disorder or agoraphobia in 17 studies met definite criteria for MVP, and 27 percent met criteria for probable MVP versus an average rate of definite MVP of 1 percent in normal controls and probable or definite MVP in 12 percent. In the 11 studies that allowed an estimate of subjects that met both auscultory and echocardiographic criteria, 10 percent of the patients with panic disorder met criteria for MVP versus 2 percent of the controls — a highly significant difference.
In a recent study (Gorman et al. 19886) with normal controls, raters blinded to psychiatric diagnoses, and severity of MVP scored as mild, moderate, and severe, 14 of 36 (39 percent) patients with panic disorder or agoraphobia met criteria for MVP versus 4 of 22 (18 percent) normal controls (p< .05). However, the MVP in the patients with panic or agoraphobia was mild and not associated with thickened mitral leaflets (the high-risk group for complications described by Nishimura and colleagues (1985) had an increase in mitral-valve thickness to 5mm or more) or small ventricular size. The authors concluded that MVP is more common in patients with panic disorder or agoraphobia, but is of doubtful significance.
Patients with panic disorder and MVP respond to antipanic drugs as well as patients with panic disorder alone (Gorman et al. 1981a; Grunhaus et al. 1984). Moreover, lactate infusion affects patients with panic disorder or agoraphobia identically whether or not MVP is present (Gorman et al. 1981&). Gorman and associates (1988&) have now reported several cases of patients with panic disorder and echocardiographically proven MVP in which the echocardiograms became normal after the panic attacks had been in remission for more than 6 months.
These findings suggest that panic disorder with MVP and panic disorder without MVP are the same illness and that panic attacks may actually be causing MVP in some patients. Gorman and colleagues (1988fr) suggested that the type of MVP seen with panic disorder is mild, much like the echocardiographic variant of normal described by Wynne (1986), and that the tachycardia and adrenergic discharge associated with panic attacks may cause a temporary anatomical deformation of the mitral valve or desynchrony in ventricular contraction sufficient to produce mild echocardiographic MVP. Experimental evidence shows that mild MVP can be induced by high heart rate and low ventricular volume (Ballenger et al. 1986) or by direct ventricular stimulation (Rosenthal et al. 1985).
Ballenger (1986) also hypothesized that high levels of circulating catecholamines in the presence of high heart rates can result in MVP. Supporting evidence for panic disorder and resulting high heart rates and adrenergic discharge causing MVP was provided by Channick et al. (1981), who found that 40 percent of patients with hyperthyroidism also had MVP.
A review of all these findings suggests that while panic disorder is associated with an increased prevalence of MVP, it seems to be a mild type of MVP that is principally an echocardiographic finding. It has little clinical relevance and does not require prophylactic antibiotic treatment. It may be caused by increased heart rate and catecholamine excretion and adrenergic tone. Weissman and colleagues´ (1987) findings supported this conclusion. They found that patients with MVP alone differed from patients with MVP and panic disorder and from patients with panic disorder alone. Patients with MVP alone exhibited more syncope, more orthostatic hypotension during quiet standing, loss of normal age-related decrease in vagally medicated heart rate variability during deep breathing, and lower 24-hour epinephrine excretion. In contrast, patients with panic attacks with or without MVP had greater increases in heart rate and mean blood pressure during each minute of quiet standing and during the early strain phase of the Valsalva maneuver.
Panic Disorder and MVPMrs. D was a 34-year – old medical student who had been having episodes of palpitations and atypical chest pain for 6 months. She had a normal physical exam and electrocardiogram, but an echocardiogram revealed mitral valve prolapse. She was treated with 50 mg of atenolol twice day, which decreased her symptoms slightly. Because of her apparent anxiety, she was referred for psychiatric consultation. On psychiatric interview, the patient revealed that her episodes of palpitations and chest pain were accompanied by dyspnea, dizziness, paresthesia, and gastrointestinal cramping. She had suffered episodes like this 5 years before and was diagnosed as having “colitis” and treated with antispasmodics. Mrs. D revealed increasing social phobias since her attacks began, with fear of crowds and of eating in restaurants. She also described her father as a nervous phobic person who never went anywhere without her mother. The patient was diagnosed as having panic disorder and mitral valve prolapse and was started on desipramine 25mg with the dosage increased to 75 mg over 10 days. She made a rapid recovery, with complete amelioration of panic attacks and the episodes of atypical chest pain and palpitations. The atenolol was successfully tapered and discontinued after 3 weeks. |
Panic disorder is frequently unrecognized in a patient with panic disorder and mitral valve prolapse. Many of these patients are prescribed beta-blockers for the MVP, which usually only mildly decrease the severe anxiety and may precipitate or worsen depressive symptoms. A switch to more specific treatment with a tricyclic antidepressant, benzodiazepine, or MAOI usually leads to rapid amelioration of panic attacks and enables the clinician to also discontinue the beta-blocker.