|
|
|
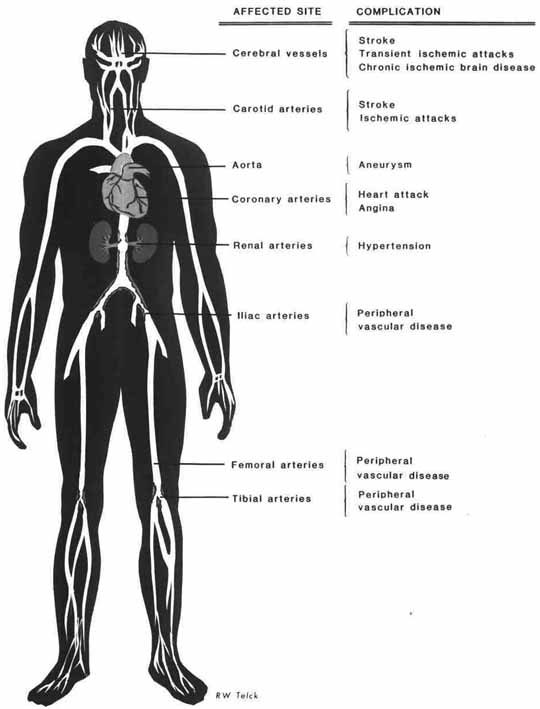
Figure 10.1 Sites for artery surgery procedures. |
| Contents | Previous | Next |
Coronary endarterectomy (Fig. 10.1) is usually confined to the right coronary artery when the artery is totally occluded, without a distal branch available for bypass. It is performed most frequently if the right coronary artery is diseased and there is stenosis of its posterior descending and distal branches. These branches are too small to accommodate a bypass. Fibrous and calcific plaques are more amenable to endarterectomy than those atheromatous in nature. The aim of surgery is to remove the entire plaque intact.
Carotid endarterectomy for removal of atheroma at the carotid artery bifurcation is a similar procedure to coronary endarterectomy. Carotid endarterectomy is becoming one of the most performed arterial surgical procedures. It is performed for symptomatic cerebral events related to the carotid bifurcation, such as transient ischemic attacks (TIAs), prolonged residual ischemic neurologic deficit (resembles a TIA but lasts for up to 48 hours), or a three-day deficit identified as a complete stroke.
Preoperatively, a computerized tomography (CT) scan is ordered to rule out brain tumor, cerebral hemorrhage, or cerebral infarction. Prior to surgery, hypertension must be under control. A light general anesthesia with entubation is preferable, but for acutely ill patients who cannot tolerate general anesthesia, a local anesthesia can be used.
Postoperative hypotension is avoided by dividing the carotid sinus nerve during the surgery. Occasionally, the blockage in the internal carotid requires a shunt around the atheroma while endarterectomy is being performed.
Carotid surgery may have complications. Rough handling can produce embolization and stroke. Lack of cerebral protection results in stroke; the use of the shunt during surgery can help to avoid this problem. Damage to nerves is another complication to be avoided. The vagus nerve can easily be caught in a clamp, which will produce a recurrent laryngealpalsy, leading to postoperative hoarseness. Damage to the hypoglossal nerve can result in transient weakness of the tongue.
|
|
|
Figure 10.1 Sites for artery surgery procedures. |
Removal of thromboemboli from an artery is termed an embolectomy. Composition of an embolus may be air, with the primary cause being fat, clot particles, or a foreign body or tumor that has lodged in a section of an artery. Diagnosis may be made by assessment of pain or numbness followed by additional signs of vascular occlusion (Section Two, Chapter 7). The artery is flushed with heparin solution and closed after the clot is removed.
Vascular reconstruction of the aortoiliac system may be accomplished with one of several procedures. Surgical removal of the intraluminal atheromatous plaque (aortoiliac-endarterectomy), insertion of a synthetic material patch, or a bypass procedure may be used. The best procedure for restoration of arterial blood flow to the leg is chosen. Thromboendarterectomy and patch grafting are chosen if the occlusive disease is limited to the aortoiliac bifurcation. With more extensive disease, a bypass graft is performed using synthetic material such as teflon or dacron. An anastomosis is performed with the proximal site in the aorta and the distal site in the common femoral of the groin. Both anastomoses are end to side with the synthetic material. When arteriography indicates that the iliac artery is relatively free of occlusive disease, the anastomosis may be proximal aorta to a distal insertion in the external iliac artery in the pelvis. Both of these procedures are almost always bilateral because of progressive disease in the other extremity. Many of the patients with aortoiliac disease also have the combination femoral-popliteal occlusive disease.8
Occlusive disease in the femoral-popliteal arteries is usually segmental. The purpose of surgery is to restore blood flow to the leg. This is accomplished via a bypass graft. The graft material may be either a saphenous vein or synthetic graft material. Success is dependent on the extent of femoral occlusion, patency of the popliteal artery, and involvement of distal arteries. There are four general classes of occlusive disease, described by degree of involvement: (1) Class I, only a segment of the superficial femoral occluded; (2) Class II, superficial femoral and popliteal segments occluded; (3) Class III, superficial femoral, popliteal, and one distal vessel occluded; and (4) Class IV, superficial femoral, popliteal, and more than one distal vessel occluded.
A good caliber long saphenous vein remains the conduit of choice for bypassing atherosclerotic obstruction of the femoropopliteal segment. Rest pain, pregangrene, and frank gangrene of the digits or forefoot in the presence of a good femoral inflow and an adequate runoff to the popliteal artery make the procedure a good risk. Intermittent claudication is a problem than can be fixed with bypass; however, good early symptomatic relief should be weighed against the risks of surgery and the uncertainty of long-term benefit.
The candidate for surgery should have given up smoking and should be symptomatic. The best candidate is one with a unilateral block, a disease-free popliteal segment, and a good caliber saphenous vein. Unfortunately, patients usually present with severe ischemia and concomitant aortoiliac or distal vessel disease. Ischemic leg ulceration, traumatic damage to the superficial femoral artery, and aneurysm of the popliteal artery are also indications for this bypass graft. Preoperative preparation includes shaving of the affected leg, the genital area, and the abdominal area to the iliac crest. Antibiotic therapy is begun 24 hours preoperatively. The shaved area is cleansed with an antimicrobial preparation the morning of and evening before surgery.
As the disease progresses, occlusion may occur in the popliteal segment and the trifurcation vessels. The patient presents with rest pain, severe ischemia, and, often, gangrene. Surgery to save the leg requires long venous grafts to the dorsalis pedis or posterior tibial arteries. Grafting is done by constructing a subcutaneous tunnel along the medial or lateral aspect of the leg and placing the vein graft in the tunnel. Longterm success rates of these grafts is about 50%. Generally, these extensive grafts are attempted in a very select patient population. Criteria for selection include severe chest pain, ischemic ulceration, or impending gangrene. An evaluation of the microcirculation is prudent also, as the patient with impeded microcirculation will frequently be a poor candidate for surgery.
Complications of femoral-popliteal bypass surgery include early graft closure, hemorrhage, infection, skin necrosis, and leg edema.
Femoral-popliteal bypass has shown excellent results in follow-up examinations, with the graft remaining patent 5-10 years after surgery.
|
|
|
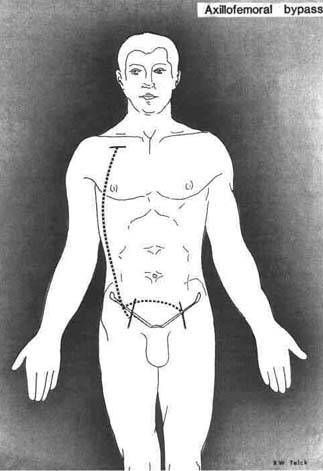
Figure 10.2 Axillofemoral bypass |
Extra-anatomic grafts (Fig. 10.2), originally designed for patients with infected grafts, poor risk patients, and elderly patients, are being used for a wider range of grafting procedures.8, 34 The axillofemoral, femoral-femoral, and obturator bypass, all of which can be performed with local anesthesia, require minimal dissection with reduced operating time. Patients with severe aortic calcification that limits the use of the abdominal aorta proximally are candidates for axillofemoral or femoral-femoral procedures. In patients with femoral to femoral grafts, the patency rate is about 90% after 3 years. The possibility of reduced flow to the donor artery must be considered because, occasionally, arm exercise reduces blood flow to the recipient extremity when the axillofemoral graft is used.
Vein grafting is the preferred technique, but synthetic materials have proven satisfactory. These grafts are becoming more popular as outcomes show that the resultant perfusion is equal to that produced by aortofemoral grafting. These grafts are usually accompanied by femoral-popliteal bypass to ensure a better runoff.
This extra-anatomic technique is indicated for restoration of lower limb blood flow when the intraabdominal route is contraindicated. If both legs are to be revascularized, axillofemoral and femorofemoral crossover grafts (axillobifemoral) are preferred to bilateral axillofemoral grafts (Fig. 10.2). The crossover graft doubles the flow in the graft and improves long-term patency. For this procedure, the first part of the right axillary artery is used as the donor artery. Because this part of the artery is fixed to the chest wall, the pull on the artery during arm movement is minimal. Another reason for choice of this artery is that the right axillary artery is less frequently impaired by subclavian atheroma as compared with the left axillary artery. Preoperatively, the brachial artery pressures should be measured and the subclavian examined for bruits. Brachial artery Doppler velocity waveforms of the brachial artery are of value, but if any doubt exists about donor artery suitability, an arteriogram is needed. Success for the graft requires a patent deep (profunda femoris) femoral artery.
In the postoperative period, antibiotic therapy in progress is continued for 48 hours. For graft patency, the patient is placed on antiplatelet therapy. Aspirin 300 mg and dipyridamole 25 mg given q.i.d. are suggested. Because the axillofemoral limb of the graft is nonpulsatile, palpation does not indicate patency.8, 17
Complications of graft are:
The most common cause of infection is a break in the sterile technique. The prophylactic use of antibiotics, very careful hemostasis, and good operating technique have reduced the incidence of postoperative complications. An infrequent complication occurring later in the postoperative period is development of a false aneurysm. Aneurysm formation that occurs in the groin may be a problem of excessive tension on the distal anastomosis, causing the suture line to rupture. Infection of any suture line may also result in aneurysm formation. This can be a life-threatening occurrence. The graft is removed, the infection is treated, and a new bypass graft is created later.
In male patients, impotency may follow aortoiliac reconstruction if there is damage to pelvic nerves and the hypogastric plexus. For young male patients, as well as the older sexually active, care is always taken when extensive dissection of the aorta and iliac vessels or surgery below the iliac bifurcation is necessary. Every attempt should be made to maximize the surgery proximal to the iliac vessels. Occasionally, potency is restored following surgery for occlusive disease.
Leg edema following femoral-popliteal bypass surgery is a frequent complication. It occurs as a result of interrupted lymphatic drainage in the femoral triangle when the saphenous vein and the femoral artery are involved. It is a temporary problem, responding to elevation.
Rupture of the aorta following blunt trauma is fatal in 80%-90% of patients. The injury may be an intimal tear with hemorrhage or a complete transection of the aorta. False aneurysm may also occur. The common symptom associated with aortic rupture following blunt chest trauma is pain, described as retrosternal and intrascapular. Assessment usually reveals a patient with dyspnea, dysphagia, cough, and hoarseness. When aortic rupture is suspected, blood pressure should be measured in both the upper and the lower extremities. The upper extremity pressure will be elevated, as is pulse amplitude. Mediastinal widening is often seen on x-ray. Repair of the aorta takes precedence over other injuries. Bypass perfusion is established with heparinization. There is the added problem of heparin with a massive bleed, but patients cannot be on the coronary bypass machine without heparinization (Chapter 11). The surgical procedure for a thoracic artery repair may employ a new innovative heparin-coated shunt, which can eliminate the use of systemic heparinization. Repair is via resection of the ruptured site with a dacron graft replacement. If the trauma site is not extensive, an end-to-end anastomosis without graft has also been advocated for repair. The use of the heparincoated bypass shunts has been significant in reducing mortality rates for these thoracic aorta repairs.
The innominate artery also is occasionally involved when trauma occurs in the aorta.2 The problem is usually close to the arch, at the origin of the artery. The lesion is often the result of a tear through the intima and medial layers, producing a false aneurysm. Rarely, the left common carotid artery and the right and left subclavian arteries are injured. Diagnosis is quite difficult. The patient presenting with a motor vehicular accident should be carefully assessed. A decrease in the distal pulse of the involved artery is one clue. Mediastinal widening viewed on x-ray is another. Emergency surgical repair is indicated to prevent hemorrhage and aneurysm formation. The site of the arterial rupture is resected, and a dacron graft replaces that portion of the artery. When possible, the patient's own vessel is repaired, anastomosed, and wrapped with tenon.
Penetrating trauma to the thoracic aorta and its major branches is a life-threatening occurrence.2 About 10% of major vascular injuries are penetrating injuries. The gunshot wound is the most common cause of these injuries, contributing 50%-70% of penetrating injuries to the great vessels. Stab wounds are second only to gunshots.
Signs and symptoms are dependent on location. Bleeding is the most common symptom. Massive hemorrhage may be the only clinical sign. Hemothorax or accumulation of blood in the pleural cavity and pneumothorax, the presence of air in the pleural cavity, may be accompanied by symptoms of hypovolemic shock (Section One, Chapter 3). If the wound has penetrated the intrapericardial segment of the vessel, the presenting symptom may be tamponade. Patients with injury to the carotid or subclavian arteries may demonstrate weak distal pulses and altered neurologic function. Assessment may also reveal symptoms of tracheal compression or congestive failure. Heart sound assessment for systolic or continuous murmurs are diagnostic near the injury site.
Emergency treatment centers on restoration of circulating blood volume and ventilation. Arteriography for the hemodynamically stable patients who can tolerate the procedure is followed with surgery. If the situation is life-threatening, diagnostic testing is not possible, and patients go directly to surgery.
The procedure of choice is dependent on the site of injury, the path of the missile, and the vessel. Vascular repair depends on the extent of injury. Minor wounds are closed and sewn. Larger wounds with blast injury may require debridement, resection, and graft or anastomosis.
Penetrating arterial wounds are frequently accompanied by venous injury. The surgical treatment usually consists of ligation or repair of the vein. Whenever possible, repair is the better treatment. Wounds of the suprahepatic vena cava are frequently associated with chest trauma. Occasionally, cardiopulmonary bypass is instituted while repair is attempted if the repair cannot be concluded with temporary occlusion of the vena cava.
Compression of adjacent structures is the primary finding as an aneurysm gradually expands. Large aneurysms may partially obstruct the left main bronchus or the superior vena cava, producing shortness of breath, venous distention of the face and upper extremities, or hoarseness due to pressure on the recurrent laryngeal nerve. Severe pain may be the result of advanced disease with nerve root compression. Large aneurysms put the patient more at risk for rupture than smaller ones. The small aneurysm is one of 5 cm or less in diameter. Surgical repair of a thoracic aneurysm is influenced by the type and location. The two types generally seen are the sacciform, in which a localized weakness results in an outpouching of the aorta wall, or the fusiform, in which the entire circumference of the aorta is involved. Surgical treatment is directed toward restoration of normal, unobstructed flow through the aorta.
A large number of aneurysms of the ascending aorta result from cystic degenerative changes in the medial layer of the aorta (Erdheim's cystic medionecrosis).34 The clinical pathology includes marked dilatation of the sinuses of Valsalva and the aortic annulus. This disease entity is called annuloaortic ectasia. Aortic regurgitation is a common finding, resulting from dilatation of the aortic sinuses and the aortic annulus (root). The leaflets cannot fall into place normally. There are several other etiologies related to ascending aortic aneurysms: arteriosclerosis, syphiliticaortitis, giant cell arteritis, trauma, aortic dissection related to hypertension, and stenotic dilatation resulting from aortic stenosis.
The patient presents with moderate to severe aortic regurgitation, the peripheral signs of widening pulse pressure with bounding pulses, and an aortic diastolic murmur. Chest x-ray often demonstrates an enlarged left ventricle and ascending aorta. Electrocardiogram (ECG) may also reveal left ventricular hypertrophy with increased QRS voltage. Aortography is diagnostic. When cystic medial degenerative disease is present, the ascending aorta and the aortic sinuses are frequently dilated. Therapy is directed toward correction of the aneurysm and the aortic valve incompetence, if this is needed. Cardiopulmonary bypass for the procedure is established, and systemic circulation is maintained until the correction is completed. The procedure calls for the pericardial cavity to be continuously irrigated with Ringer's solution at 4°C. A potassium-containing solution of 30 meq/L, also at 4°C, is injected directly into the coronary ostia at 20- to 30-minute intervals to maintain cardiac arrest. The myocardial temperature is kept below 18°C. The supracoronary graft procedure involves replacement of the ascending aorta from the level of the aortic commissures to a site proximal to the origin of the innominate artery. The aortic valve is then replaced. The diseased aortic wall is excised with aortic valve leaflets intact. A prosthetic valve is inserted, and a low-porosity dacron graft is sutured to the proximal aortic cuff and then to the distal aorta.
Another procedure calls for a total prosthetic replacement of the ascending aorta and the aortic valve—a combined replacement procedure.14,34 There are advantages and disadvantages to both techniques. With the supracoronary graft and valve replacement, there are no coronary anastomoses, but the complications include bleeding, leaking, and possible later development of an aneurysm of the sinus of Valsalva. The combined replacement graft has the advantages of excision of all abnormal aorta with no bleeding through graft or distal suture line. The disadvantages include the possibility of graft compression, stenosis of coronary arteries, and formation of pseudoaneurysms at coronary and distal aortic anastomoses.
The surgical treatment for the problem of cysticmedial disease with dilatation of the sinuses of Valsalva is a combined replacement graft of the ascending aorta and aortic valve. Supracoronary graft replacement of the aorta, followed by aortic valve replacement, is the preferred technique for aneurysms not associated with cystic disease or Valsalva aneurysms.
Complications of both techniques include heart block, thromboembolic problems, anticoagulant therapy leading to hemorrhage, myocardial infarction, congestive failure, and life-threatening dysrhythmias.
Aneurysm of the transverse arch usually affects only the aortic wall, leaving orifices of the great vessels free of disease. Reconstruction encompasses reimplantation of the great vessels as a unit into a new dacron arch graft. This procedure is highly successful, and it reduces the possibility of postoperative bleeding or thrombosis on an arch vessel.
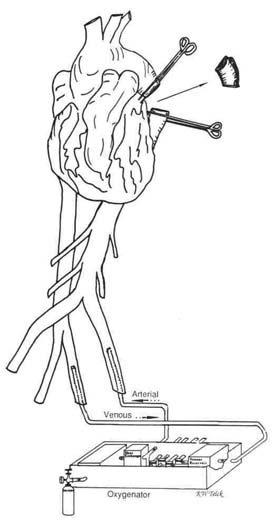
The principal concern with a descending aortic aneurysm is the prevention of ischemic injury to the spinal cord. Spinal cord perfusion is highly variable, including the intercostals, the left subclavian, and the thoracic aorta. Several cardiopulmonary bypass techniques are used for this surgical procedure. Atrialfemoral bypass using the bypass pump to provide circulation to the abdominal aorta (Fig. 10.3) is one technique. Femoral artery to femoral vein with an oxygenator in the circuit is another. This newer technique involves expeditious removal of the aneurysm with replacement of the descending thoracic aorta using the femoral-femoral without a pump. Heparin, usually 1 mg/kg body weight is used. The activated coagulation time (ACT) is maintained above 400 seconds to prevent clotting. Reversal is accomplished with protamine to the preheparin ACT of 100-120 seconds. This will prevent microemboli from occurring from the short period of aorta clamping.
|
|
|
Figure 10.3 Oxygenator bypass for aortic surgery. |
During the course of the procedure, blood pressure is checked frequently to avoid excessively high or low pressures proximal to the clamp. Additionally, left atrial pressure is measured to avoid overloading the left ventricle, which would lead to pulmonary edema. The right radial artery is used to determine pressures because the left subclavian is usually clamped during the repair. Descending aortic aneurysms usually extend from the subclavian to the diaphragm. After excision, the graft is sutured in place, air is expelled, the clamps are removed, and the bypass perfusion is discontinued.
Dissecting aneurysm is the splitting of the intima of the aorta, which permits blood to pass between the layers of the wall, forming a false channel. It is a common problem involving the aorta. The origin of the dissection is usually in the ascending aorta or just distal to the left subclavian artery.17 It is infrequently found in the arch of the aorta. At times, diagnosis is not made until the aneurysm extends to all segments of the thoracic aorta and the abdominal aorta. Dissection rarely originates in the abdominal aorta.
The patient presents with sudden onset of severe pain, unrelated to exertion, anteriorly or in the intrascapular area. The pain is described as tearing, cutting, or stabbing, and it is unrelieved by rest, rdtroglycerin, or opiates. The onset is dramatic to the point of hospital admission for acute myocardial infarction. The pain persists despite medication. Chest x-rays show a widening mediastinum, which can be diagnostic when accompanied by aortogram. The origin of the dissection can be identified.
For acute aneurysms of the ascending aorta, diagnosed by the presence of aortic regurgitation or the reduction of pulses in one of the aortic arch vessels, immediate surgery is indicated to prevent aneurysm rupture. An aortogram is not always useful in this diagnosis because the catheter may enter the false lumen.
Injection of the dye will increase the dissection, perhaps causing it to rupture. In addition to ascending aortic aneurysm, surgical intervention for dissecting aneurysm is indicated for aortic valve insufficiency; rupture into the pericardium; occlusion of the arch vessels; descending aortic aneurysm; occlusion of the celiac, renal, or iliac arteries; and combinations of these problems.
The threat of rupture is not as great in descending aneurysms. The presence of paraplegia or pulseless lower extremities is the indicator for immediate action.
Chronic dissecting aneurysms are handled surgically in the same fashion as fusiform aneurysms. Only when the lesion is confined to the descending aorta alone is the entire section excised and replaced with a graft.
The guidelines for surgical intervention can be described as twofold. For acute dissections:
For chronic dissection two-week onset:
Ventricular aneurysms usually occur in conjunction with myocardial infarction. Other causes such as hypertrophic cardiomyopathy, mitral valve problems, trauma, and sarcoidosis have occasionally been suspect in the development of a ventricular aneurysm. The infarction, with necrosis of the myocardium and associated pericarditis, causes pericardial adhesions to develop. In the 10-14 day period following the acute event, the free wall of the ventricle may rupture. One of three types of aneurysm may result. A false aneurysm may develop from a small section of ruptured free wall of the infarcted ventricle. The false aneurysm develops as a result of an incomplete rupture whose hole seals itself with thrombotic material and pericardial adhesions. These aneurysms are composed of pericardium and thrombus without myocardial tissue. False aneurysms rupture more readily than true aneurysms. A true aneurysm of the ventricle has near-total fibrous tissue replacement of the infarcted muscle. The necrotic muscle becomes a thin-walled, well-demarcated fibrous sheath, subjected to high pressure. This segment of the ventricle dilates, forming a noncontractile fibrotic sac that bulges out as a separate chamber during systole and diastole. Most true aneurysms are located in the anterior apical region. Thrombi often develop as a result of stasis of blood. Further complication occurs if the papillary muscles of the mitral valve lie in the ventricular wall section in which the aneurysm occurs. A mitral regurgitation may occur due to traction on the valve by the aneurysmal sac.
Functional aneurysm is the third type of ventricular aneurysm, differing from a true aneurysm in that the true aneurysm bulges during systole and diastole, but a functional aneurysm protrudes only during systole. It is sometimes difficult on angiography to distinguish a functional aneurysm from a small true aneurysm.
All aneurysms interfere with effective contraction of the left ventricle, reducing cardiac output and creating paradoxical movement. The resultant left ventricular enlargement increases wall tension and oxygen demand. Left ventricular end diastolic pressure becomes elevated when the aneurysm retains 15% or more of the end diastolic volume.
Patients presenting with congestive failure, angina pectoris, ventricular tachyarrhythmias, and systemic emboli are candidates for resection of the aneurysm. Patients who are asymptomatic are not necessarily surgical candidates. The status of the residual myocardium must be taken into account to determine if the surgical intervention will alleviate the problem.
Aneurysms of the abdominal aorta have atherosclerotic origins. The majority arise below the renal arteries and terminate at the bifurcation of the aorta or common iliac arteries. The aneurysm disease may involve the distal aorta, but occlusive disease may exist in the iliac arteries, requiring resection or bypass of these arteries as well as restoration of perfusion. Any combination of arteries may become involved in the aneurysm disease: the renal arteries or the internal or external iliacs below the bifurcation of the common iliac. The majority of abdominal aortic aneurysms are localized to distal abdominal aorta and proximal common iliac arteries.
Abdominal aneurysm is frequently discovered accidentally. Often the mass exists without symptoms. A pulsatile mass with severe back and abdominal pain suggests impending rupture. Rupture may occur into the peritoneal cavity, the retroperitoneal space, or the vena cava. Surgical treatment for abdominal aorta aneurysm is excision and synthetic graft replacement.
Nursing ManagementPriorities for care of a patient undergoing arterial surgery are:
Nursing Diagnoses Most Frequently Associated with Arterial Surgery
|
| Table 10.1 Nursing Care Plan for the Patient with an Aortic Aneurysm Repair | |||||
| Nursing Diagnosis | Assessment Data | Expected Outcome | Nursing Interventions | ||
| 1. | Alteration in comfort; pain related to surgical procedure. | Subjective data: Patient states, "My operation hurts; I cannot find a comfortable position; the tube in my chest is pulling" Objective data: Facial expression reveals discomfort and anxiety Elevated blood pressure Restless behavior, moves about in bed frequently Diaphoretic |
The patient will maintain comfort level, will be free from pain. | 1. | Auscultate abdomen for bowel sounds |
| 2. | Observe for nonverbal signs of pain at least q. 1-2 h. | ||||
| 3. | Provide pain medication as needed. | ||||
| 4. | Evaluate results of pain medication. | ||||
| 5. | Provide quiet environment for rest. | ||||
| 6. | Check operative area for signs and symptoms of edema, inflammation. | ||||
| 7. | Position for comfort. | ||||
| 2. | Alteration in tissue perfusion: peripheral related to low circulating blood volume. | Subjective data: Patient states it is difficult to stay awake States he has little energy to perform activities of daily living States he is cold and requests more blankets Objective data: Decreased peripheral pulses Edema of extremities Extremities cold to touch Mottled appearance of lower extremities Confusion about time, date, place Reduced urine output |
The patient will maintain adequate tissue perfusion (e.g., stable circulatory status, normal vital signs, adequate output). | 1. | Assess peripheral pulses frequently, bilaterally. |
| 2. | Monitor neurologic status. | ||||
| 3. | Monitor extremities for color, warmth, turgor. | ||||
| 4. | Monitor motor reflexes. | ||||
| 5. | Monitor and record dysrhythmias. | ||||
| 6. | Measure and record output. | ||||
| 7. | Assess heart and lungs. | ||||
| 8. | Weigh daily. | ||||
| 9. | Position relatively flat. | ||||
| 3. | Impaired gas exchange related to oxygen deficiency. | Subjective data: Patient states he is short of breath; says he is frequently confused Patient relates that he is restless Objective data: Tachycardia Abnormal blood gases Mentation is altered, patient is confused Uses accessory muscles for inspiration Intercostal retraction Cyanotic nailbeds, lips |
The patient will maintain normal oxygen levels | 1. | Turn q. 2-3 h. |
| 2. | Suction as needed. | ||||
| 3. | Maintain patent airway. | ||||
| 4. | Monitor Arterial Blood Gases. | ||||
| 5. | Monitor and record vital signs q. 2 h. | ||||
| 6. | Monitor sensorium q. 2 h. | ||||
| 7. | Teach importance of cough and deep breathing. | ||||
| 8. | Record respiratory effort, chest excursion. | ||||
| 9. | Use incent spirometer as soon as feasible. | ||||
| 10. | Assess lung sounds frequently. | ||||
| 11. | Assess for signs of central and peripheral cyanosis (nailbeds, lips, earlobes). | ||||
| 12. | Report results of chest x-ray. | ||||
| 4. | Fluid volume deficit related to blood loss during surgery. | Subjective data: Patient states, "I need water, my mouth is dry; I am cold" Objective data: Reduced urine output Dry mucous membranes Thirst present Coated tongue Weight loss Diminished bowel sounds |
The patient will maintain fluid output equal to or greater than 2/3 of intake. The patient will maintain a urine output of 30 ml/hr or greater. | 1. | Measure and record urine output q. h. |
| 2. | Measure and record chest tube drainage q. 8 h. | ||||
| 3. | Monitor and assess vital signs q. 2 h. | ||||
| 4. | Assess for retroperitoneal area drainage. | ||||
| 5. | Check all dressings frequently for drainage. | ||||
| 6. | Monitor and record all pulses q. 2 h. | ||||
| 7. | Monitor skin color, temperature. | ||||
| 8. | Monitor electrolytes. | ||||
| 9. | Observe for signs and symptoms of dehydration. | ||||
| 10. | Assess abdomen for girth and bowel sounds. | ||||
| 11. | Maintain patent IV. | ||||
| 12. | Offer food and fluid as tolerated. | ||||