|
|
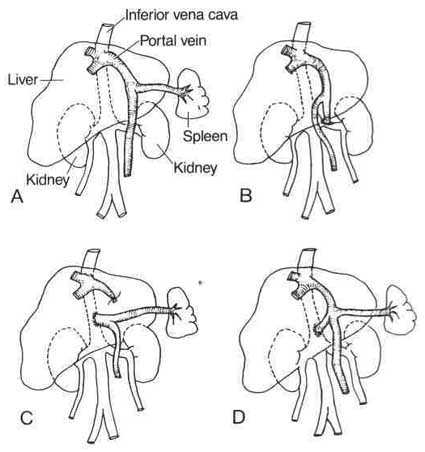
| Figure 9.1. A. Normal liver with normal blood flow. B. End to side spelnorenal shunt. C. End to side portacaval shunt. D. Mesocaval H-graft shunt |
| Contents | Previous | Next |
Varicose veins, dilated superficial veins of the legs, become a surgical problem when complicated by chronic venous insufficiency or recurrent attacks of thrombophlebitis. Surgical treatment of varicose veins in the past has been less than successful. This may be due to the outdated concept that the problem lies with primary valvular incompetence. Operative techniques have concentrated on ligation of main stem superficial veins and/or ligation of incompetent deep veins (Table 9.1). Full-length stripping has not been completely successful because of failure to remove varicose branches.
Newer concepts of cause suggest that the primary lesion is in the muscle and elastic layers of the vein wall. A degenerative fibrosis develops, which produces dilation not only of the vein wall between the valves but of the valve ring itself. There dilation creates a secondary valvular incompetence because the valve cusps cannot close properly and eventually atrophy through disuse.34 This degenerative process affects both the deep and the superficial veins.
Surgical treatment for this problem is removal of the varicose veins combined with proximal ligation at the main saphenofemoral or saphenopopliteal junction, wherever incompetence exists at these points. Removal of the superficial varices and the junctions makes it unnecessary to ligate the deep veins because drainage into the superficial veins will be eliminated by their removal.
Thrombophlebitis or phlebothrombosis involving the iliofemoral region presents a problem for blood flow. If thrombosis occurs, the clot occludes circulation. A surgical procedure, venous thrombectomy, is the procedure of choice to remove the clot.
| Table 9.1. Venous Ligation |
|
Preoperative Indications for venous ligation surgery
|
Other than those originating in cardiac chambers, most thromboemboli originate below the level of the vena cava. When anticoagulation therapy is not an option or is not effective in the prevention of embolism, the surgical approach is focused on trapping emboli in the inferior vena cava.9, 34 The procedure used in the past, ligation of the vena cava, has fallen into disfavor. High mortality rates, recurrent embolism from unfiltered collaterally developed veins, and postphlebitis stasis sequelae led to the development of newer techniques. Several vena caval filtration techniques evolved. Vena caval patency is retained while clots are filtered. Patients who continue to have pulmonary emboli in spite of adequate anticoagulation are candidates for interruption of the vena cava. Also considered as candidates are patients with venous thrombosis when anticoagulation is contraindicated (for example, patients with neurologic disease, neurosurgery, and some types of ophthalmic disease). Patients with compromised respiratory systems from other lung diseases or pulmonary emboli are candidates for the procedure.
There are several methods for interrupting the inferior vena cava.34 The transvenous approach has many advantages over an abdominal approach for the acutely ill patient. Techniques include the MobinUddin umbrella, the Hunter balloon, and the Greenfield filter. The Greenfield filter has several advantages, including low recurrent embolism rate, better long-term inferior vena caval patency, and a lower tendency to filter migration.
Surgical shunting procedures for obstruction of the portal system, either intrahepatic or extrahepatic, decrease portal hypertension by diverting some of the portal blood flow (Fig. 9.1A). Thrombosis is frequently the cause of extrahepatic obstruction. Shunting between the hypertensive portal system and the lower caval circulation relieves the portal pressure and brings relief to esophageal varices. Several approaches are used for portosystemic shunting: splenorenal (Fig. 9.1B) anastomosis between either the proximal or distal splenic vein and the left renal vein, portacaval anastomosis between the portal vein and the inferior vena cava (Fig. 9.1C), or a mesocaval shunt (Fig. 9. ID), in which a short dacron prosthetic graft is placed between the superior mesenteric vein and the inferior vena cava.
|
|
| Figure 9.1. A. Normal liver with normal blood flow. B. End to side spelnorenal shunt. C. End to side portacaval shunt. D. Mesocaval H-graft shunt |
Frequent complications follow shunt procedures. Hepatic encephalopathy is a common problem. The shunt diverts ammonia from its normal path of entry into the liver, going instead into systemic circulation.
Nursing ManagementPriorities for nursing care of a patient undergoing venous surgery are:
Nursing Diagnoses Most Frequently Associated with Venous Surgery
|