|
|
|
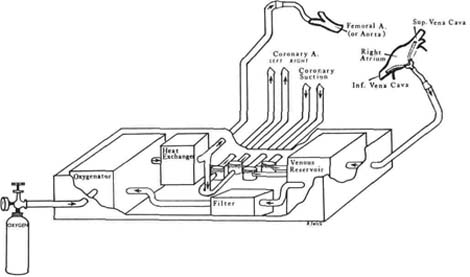
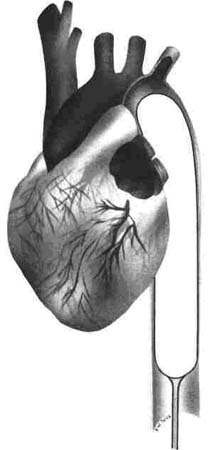
Figure 11.1 Cardiopulmonary bypass machine. |
| Contents | Previous | Next |
The preoperative phase for the cardiovascular surgical patient, regardless of procedure contemplated, begins prior to hospital admission or with the admission. This phase involves correcting any other health problems, stabilizing problems that cannot be eliminated (e.g., diabetes, hypertension), and optimizing cardiovascular function.
The preoperative nursing assessment should include:
Preoperative care includes therapy for potential or actual problems, such as infection, dysrhythmias, fluid and electrolyte imbalance, and any cardiac problems, such as congestive failure, that are identified. The admission nursing assessment should include an evaluation of the patient's anxiety levels. Questions about patient knowledge of the planned procedure are included in the assessment in preparation for patient and family education. The first encounter, when rapport is developed with patient and family, is an excellent time for this assessment. A trusting relationship between the nurse and the patient is developed when the nurse responds to questions with honest answers and information to clarify misinformation, listens to expressed fears and concerns, and prepares the patient for the hospital routines. The preoperative teaching helps to decrease anxiety levels.
This phase of preoperative education should be based on an assessment of learning needs as well as on the information that has already been given prior to admission by the physician. Reinforcement is often required.
It is the physician's responsibility to inform the patient realistically about the disease state, the need for the surgical procedure, the risks involved, and the expected outcome. Patients who are prepared with correct information manifest less anxiety. Explanations and reassurance can be used to reduce anxiety levels. Weak assurances such as "Everything will be just fine," are not realistic or helpful to patients. This is a promise that may not prove possible.
Nursing intervention is directed toward reinforcing correct information, correcting misinformation, and adding to the patient's knowledge. When describing the actual procedure, the use of models, diagrams, and audiovisual aids will frequently clarify information, particularly when explaining anatomy. If specialized equipment will be used, such as the cardiopulmonary bypass machine, an explanation of how it operates and the relationship to postoperative monitoring of coagulation time, fluids, and blood studies may be in order. Any description of the surgical procedure should include a description of the actual incision. The patient experiencing a bypass procedure should be made aware that the sternum will be opened and closed with wire that will remain in place. Varicose vein ligation incisions, thorocotomy incisions, or abdominal incisions should be described. The patient has the right to know what to expect. Teaching for the postoperative care period can be more easily understood and accepted if the procedure is described. The importance of coughing and deep breathing, the control of pain, tubes and drains, fluid replacement, and other details can be discussed to relieve the patient's anxiety and increase the knowledge base.
Nursing ManagementPriorities for preoperative nursing care of a patient scheduled for a cardiovascular surgical procedure are:
Nursing Diagnoses Most Frequently Associated Preoperatively with Patients Scheduled for Cardiac Surgery
|
Early recognition of complications or potential complications and the promotion of a therapeutic environment is essential for optimum patient recovery.
An initial systems assessment postoperatively establishes a baseline for care. Hemodynamic parameters are recorded and the pulmonary, renal, and neurologic statuses are evaluated and documented. If applicable, a hematologic assessment is included. ECG reports and chest x-ray examinations may be ordered.
Cardiopulmonary bypass, also called extracorporeal circulation, is a technique in which blood is diverted away from the heart and lungs into a machine (Fig. 11.1) that substitutes for the pumping and ventiatory functions of these organs. Both heart and lungs are bypassed. Stated simply, the machine drains blood from the heart, oxygenates it, and pumps it back into the body. Blood is drained from the heart by a venous cannula placed into the right atrium or by cannulas placed into the inferior and superior vena cavae. The vena caval approach is used if the surgical procedure is to the right atrium, the right ventricle, or the pulmonary arteries. For surgery to the aorta, coronary bypass, or aortic valve, the right atrium is cannulated. Blood from the coronary sinus is stopped by a clamp on the aorta. Cardiac arrest is then produced with cold cardioplegic solutions of potassium chloride. Complete bypass means that the entire systemic venous return to the heart is collected and delivered to the oxygenator by gravity drainage. The venous reservoir is positioned about 30 inches below the level of the right atrium to ensure total diversion. This blood is filtered, passed to the oxygenator, and then to the heat exchanger. Cannulation of the ascending aorta for arterial return is the favored site. In patients with surgery of the left heart or those with a disease process that prevents use of the aorta, a femoral artery inflow is used. When satisfactory venous outflow and arterial inflow occur, total cardiopulmonary bypass is accomplished. Many procedures include cross-clamping of the ascending aorta as well, before surgery is begun. This seems to avoid the occurrence of systemic and cerebral air embolus. There are several possible postoperative problems that can occur when the patient is taken off bypass. Hemolysis, trauma to the blood due to the pumping action of the machine, occurs because blood in contact with surfaces other than natural conduits alters blood elements. Longer periods on the bypass machine create more problems. Heparin rebound is also a problem. Blood contact with extracorporeal surfaces activates the coagulation system. Heparin inhibits factors V, IX, XI, and XIIa and thrombin, but it is required to prevent coagulation during bypass. Commonly, 3 milligrams of heparin per kilogram of body weight is given initially, followed by adequate heparin to maintain the activated coagulation time (ACT) above 8 minutes. After bypass, protamine sulfate in amounts of 3/4 to 11/2 milligrams per milligram of administered heparin is given intravenously over a 10-15 minute period to avoid a hypotensive reaction. The rebound of heparin to circulation in the postoperative period is possibly due to the differing metabolism rates of the two drugs.
|
|
|
Figure 11.1 Cardiopulmonary bypass machine. |
Transient neurologic problems may occur following bypass due to microemboli, hemodilution, and fluid shifts. This is usually a transient problem.
For many types of cardiac surgery, a heart that is stopped is preferable to one that is beating. Extreme cold and hyperkalemia are agents for rapid cardiac arrest. Cardioplegia has been refined from the use of potassium citrate solutions and acetylcholine to a technique of cold cardioplegia induced with a mixture of 500 milliliters of 5% dextrose and 0.45% NaCI at a temperature of 6°C and a solution of potassium chloride, magnesium chloride, calcium chloride, and bicarbonate. The solution is refrigerated to 4°C and injected into the aorta root or perfused directly into the coronary ostia in 500 cc increments. Each increment is sufficient to produce asystole for one hour. Additionally, to ensure cardiac hypothermia, a cold solution of Ringer's solution is poured over the epicardium.
Introduction of several innovations has enhanced the technique for direct coronary artery surgery with complete revascularization—coronary artery bypass grafting (CABG).8 Cold chemical cardioplegia, disposable pump lines and oxygenators, optical magnification, microsurgical instruments, and cold headlight illumination are just a few of the innovations in cardiac bypass surgery that make the procedure available even to patients with unstable angina and left main coronary artery disease.
Coronary artery distribution must be ascertained before bypass surgery is undertaken. The dominant right coronary system, the most commonly found type, is one in which the right coronary artery is responsible for circulation to the posterior heart, both left and right ventricles, and the interventricular septum. The dominant left coronary system is one in which the circumflex branch of the left coronary artery is responsible for circulation to the posterior left ventricle and the septum. In some patients, both right and left coronary arteries have posterior descending branches of equal size. The anastomosis to the coronary arteries is dependent on size and dominance of the arteries. If the posterior arteries to be used for anastomosis are severely diseased, an endarterectomy is performed prior to the insertion.
The saphenous vein is the preferred one for aortocoronary bypass. If unavailable, the cephalic or basilic veins may substitute. Use of the internal mammary artery is an earlier technique now being revitalized.
Following excision of the saphenous vein, the patient is placed on bypass, and hypothermic cooling is instituted. This reduces myocardial oxygen demand. Cardioplegia reduces metabolic demand and allows the surgery to be performed in a bloodless field with the heart at standstill.
A sequential graft, using one vessel to bypass several occluded areas, is often used when more than one coronary vessel is occluded. This type of graft is ideal for multiple bypass grafts in the same or more than one vessel. The sequential graft requires fewer anastomoses, which is a definite advantage.
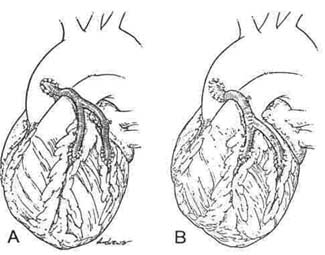
Another technique—a "Y" graft (Fig. 11.2)—is initiated when a bypass graft is to be performed but there is a short supply of graft material. This procedure calls for the fashioning of a Y with the usual proximal and distal anastomosis between the aorta and the diseased coronary artery. A second occluded artery can be bypassed by making another proximal insertion for the second bypass directly into the first vein graft rather than the aorta. The distal anastomosis, as usual, bypasses the occlusion.
|
|
|
Figure 11.2 Example of Y vein grafts. |
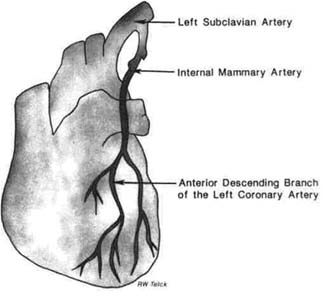
When the internal mammary artery is anastomosed to a coronary artery, the same procedure is used as for anastomosis of the saphenous vein (Fig. 11.3).
|
|
|
Figure 11.3 Internal mammary artery bypass graft. |
Following the completion of the grafting, the patient is weaned for cardiopulmonary bypass, and the heart is started.
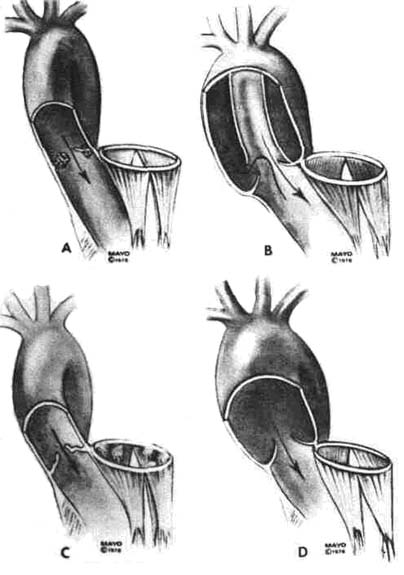
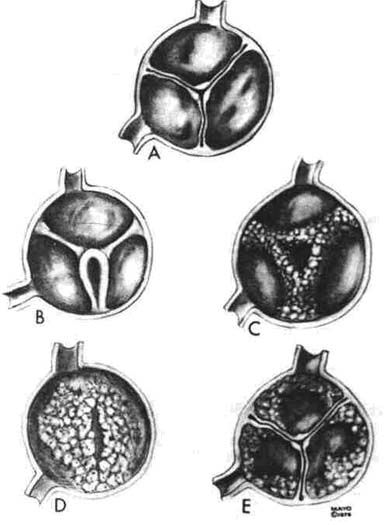
Diseases of the aortic valve, congenital, acquired, or incompetent (Fig. 11.4), are common. The patient with aortic insufficiency may be asymptomatic for years. Aortic stenosis, following a latent asymptomatic period, may dramatically display classic symptoms of angina, syncope, and congestive failure. Patients with these symptoms of aortic stenosis (Fig. 11.5) should be considered for valve replacement.13 An incompetent valve is also a candidate for replacement.
|
|
Figure 11.4 Types of aortic incompetenc. |
Figure 11.5 Type of aortic valvular syenosis. |
In the adult patient, aortic valvotomy of valvoloplasty is not feasible or successful. Valve replacement is the technique of choice. Resection of a fibrotic valve is not as difficult as replacement of a heavily calcified one. The diseased valve is excised, and a prosthetic valve is placed. The surgery is necessarily quite delicate to avoid damage to the atrioventricular (AV) bundle lying near the aorta cusp. Air is evacuated from the ascending aorta, followed by closure. The ideal valve has yet to be invented.
A prosthetic valve should be:
Two types of valves are available: mechanical and biological. The caged ball principle is widely used for mechanical valves. The porcine (pig) valve approximates the human valve and is the one most frequently used.
Biological valves in use today are:
Lesions of the mitral valve may be stenotic, regurgitant, or combinations of both. Rheumatic fever is the usual major cause of acquired mitral valve lesions, although other etiologies such as bacterial endocarditis, ruptures, chordae tendineae, and ischemia related to myocardial infarction also produce a resultant valvular incompetence. The major problems of the mitral valve are (1) fusion or thickening of the commissures; (2) fusion or shortening of the papillary muscles or the chordae tendineae; or (3) calcification of the leaflets. The fusion and calcification changes may result from turbulent blood flow, adding to the fibrosis and calcification, which in turn raises the level of turbulence. Commissurotomy is the treatment of choice to interrupt the cycle. Commissurotomy is the surgical procedure that separates the adherent, fibrotic leaflets of the mitral valve.
Mitral stenosis, the most common of the lesions,22 progresses to a point where the mitral valve is reduced to a slit opening through the fibrotic plaque, limiting forward flow into the left ventricle. The reduced flow raises pressure in the left atrium, the pulmonary vascular bed, and, eventually, the right side of the heart. The patient presents with a characteristic diastolic murmur. Commissurotomy may be performed as a closed technique—without bypass—or as an open procedure. The generally accepted procedure today is the open technique with cardiopulmonary bypass, which permits better visualization to remove left atrial thrombi, as well as a more accurate surgical approach to open the commissures widely and repair fused chordae or papillary muscles. Calcium deposits can also be removed to improve valve mobility.
Mitral regurgitation, another common lesion, is frequently the result of a dilated mitral annulus (ring)22 in combination with myocardial ischemia following infarct or a prolapsed posterior leaflet accompanied by ruptured chordae tendineae. Residual damage from rheumatic fever produces fibrosis of the leaflets with deformity that does not permit normal closure during the systolic phase of ventricular contraction. The preferred surgical treatment for a simple regurgitant valve disease is valve annuloplasty. The circumference of the mitral annulus is reduced so that the leaflets fall into place again.
Mitral valve replacement is the excision of the mitral leaflets, the chordae tendineae, and the papillary muscles to be replaced by a prosthesis, either mechanical or biological.
Acquired tricuspid valve disease is uncommon. Stenosis or insufficiency may be a residual of rheumatic fever. This valve is rarely diseased without mitral or aortic involvement.
Ventricular assistance34 is defined as unloading one or both ventricles by shifting the blood volume. Use of a ventricular assist device is indicated when there is cardiac failure postsurgery and when medications and the intra-aortic balloon pump (IABP) do not succeed in weaning a patient from bypass. The right ventricular assist device (RVAD) is used for general heart failure. A left ventricular assist device (LVAD) (Fig. 11.6) or biventricular (BVAD) assist device provides cardiac assistance by means of artificial ventricles, driven mechanically or pneumatically. A LVAD is implanted between the left atrium or the left ventricle and the aorta. The artificial blood pump works parallel to the natural heart. Access can be via the left atrium or the left ventricle. The ventricular access is superior as blood is directed by the pump to the ascending aorta, producing direct high perfusion of the heart, or to the thoracic aorta and the abdominal aorta, producing pulmonary and renal artery perfusion.
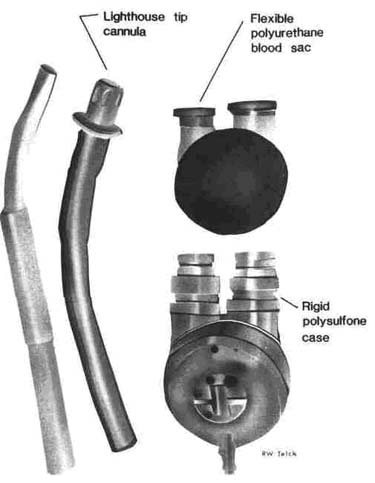
The clinical assist device (left ventricular assist) consists of a flexible polyurethane blood sac and diaphragm within a rigid case. A cannula is inserted into the left ventricular apex and secured in place with pledget-supported sutures. Inlet and outlet disc valves are used in the device to provide unidirectional flow. Pumping action is generated by a pneumatic power unit that pulses the flexible sac to periodically compress the blood sac. An example is Novacor's pulsemaker (Fig. 11.7). The pump produces a stroke volume of 65 ml, with a maximum output of 6.5 L/m. A power unit activates the blood pump. Blood return is achieved through a dacronprosthesis anastomosed to the ascending aorta.
When a right ventricular assist device is required, the implantation is between the right atrium or right ventricle and the pulmonary artery. For ventricular access, a transatrial access through the tricuspid artery is used. Although still very experimental, results thus far have demonstrated:34
Patients with end stage cardiac disease following coronary artery disease (CAD) or cardiomyopathy and patients with failure following a myocardial infarction (MI) are also candidates for implanted VAD. A temporary ventricular assist device is implanted via a cardiac surgery procedure.
Ventricular assist devices may be implanted in the following patients:
The following problems are encountered with VAD implants:
|
|
Figure 11.6 Left ventricular assist device. |
New surgical options have provided modalities of therapy that were not previously available to patients with drug resistant ventricular tachycardia. Two new options are resection of irritable foci34 and electrical intervention using the automatic internal cardioverter defibrillator (AICD).
Usually a patient with a large, easily resectable ventricular aneurysm with recurrent tachycardia is resistant to drug treatment. Surgical technique consists of epicardial and endocardial electrophysiologic mapping of ventricular tachycardia during normothermic cardiopulmonary bypass. The site of origin is identified, the aorta is cross-clamped, and cold cardioplegia is instituted. An endocardial resection is carried out, including the site of the arrhythmia and a 2-3 cm margin on all sides. Some patients require CABG, mitral valve replacement, and implantation of an AICD in combination with this procedure.
Ten days following the resection, patients undergo repeat electrophysiologic provocative testing to check for sustained ventricular tachycardia.
|
|
|
Figure 11.7 Navacor's pulsemaker. |
Electrical intervention for the patient resuscitated from an episode of sudden cardiac or sustained ventricular tachycardia also appears to be successful when a drug regimen cannot be established. A promising intervention has been the automatic implantable cardioverter defibrillator (AICD). This device senses arrhythmias by heart rate and the probability density function. It is necessary for both criteria to be satisfied before the device will fire.
The rate detection circuit senses a sustained heart rate above a preset value (usually 155 bpm). The rate •criteria alone will not fire the device. Rate criteria alone does not differentiate supraventricular tachycardia (SVT) from ventricular tachycardia (VT).
The probability density function distinguishes VT or ventricular fibrillation (VF) using a criterion of the amount of time the QRS complex is away from the isoelectric line. In sinus rhythm or SVT, the QRS complex remains on the isoelectric baseline. Wide complexes of VT or coarse VF are frequently above the baseline. This is sensed and, along with advanced rate, will fire the cardioverter defibrillator. There are rate-only models available also. These units will shock any rhythm above the set rate. For most models of AlCDs, 5-20 seconds are required to sense VT or VF, with 5-15 seconds required to charge its energy storage capacitors. The first shock delivered varies between 23 and 28 joules. If unsuccessful in converting the heart rate, second, third, and fourth countershocks are delivered with intensity increasing from 28 to 37 joules. A detection and charging period of 10-35 seconds occurs between shocks. Four shocks is the maximum that the unit can deliver; it will not recycle after that number. The electrodes and the AICD unit are placed in the operating room with the patient under general anesthesia. Three types of leads are placed to make the unit workable.
Cardiac transplantation has been established as a treatment modality for patients with end state CAD, cardiomyopathy, untreatable congenital cardiac diseases, and cardiac tumors. The primary indication is the patient with severe cardiac failure as a result of irreversible left ventricular muscle disease due to ischemic heart disease or congenital cardiomyopathy. Ideally, the candidate for transplant would be under age 50, with a pulmonary artery pressure less than 40 mm/Hg; infection-free; nondiabetic, with no recent history of pulmonary embolism or infarction; and with no other incurable illness. The addition of cyclosporin to the drug regimen of the transplant patient has sharply increased the survival rate in the past few years. The number of cardiac transplant procedures performed has increased tremendously.6, 8
ABO blood group compatibility between donor and recipient is essential, as is a negative lymphocyte cross-match if the recipient has preformed cytotoxic antibodies. The problem of adequate supply of donors remains. Advances in preservation of donor organs has meant it is now possible to acquire organs from areas in a 500-mile radius of the transplant center.
Donor candidates must of necessity be young men under age 35 and women under age 40. The prevalence of undiagnosed coronary disease in the population as a whole puts this limit on donor organs. Another problem that occurs when older donor hearts are used is that graft arteriosclerosis tends to accelerate more rapidly in recipients of hearts from donors older than age 35. Size compatibility between donor and recipient is also important.
Rejection and infection are the greatest threats to the transplant patient. Normal defenses are impaired by the high dosages of immunosuppressants required to prevent rejection.
The IABP, the left and right ventricular assist pumps, and the pneumatic artificial heart represent a range of devices capable of keeping a patient alive while awaiting a donor heart. The major problem in the use of any of these is infection.
|
|
Figure 11.8 Experimental permanent implantedLVADs. |
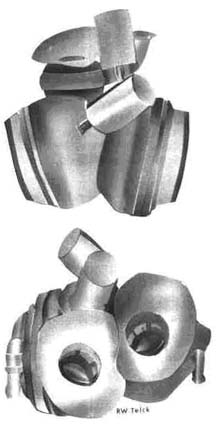
Pneumatic artificial heart, another device, one of which is the Pennsylvania device, (Fig. 11.8), consists of two separate prosthetic ventricles, each similar to the VAD. Each of the prosthetic ventricles is attached to a natural atrial remnant and to the great vessel. Atrial cuffs made of a special fabric are used. Dacron vascular prosthesis interfaces the outlet part of the ventricle to the great vessel. The blood sac fills with blood and empties by pulses between the sac and its rigid housing. Unidirectional valves are used (BjorkShiley prosthetic valves). The pneumatic power units are in a separate console and supply the pulses to the artificial heart by way of large bore percutaneous tubes. The tubes are tunneled subcutaneously in the transthoracic region. Each ventricle is driven by a separate power unit.
Over the last 10 years, a great deal of progress has been made in the development of devices to supply circulatory support. The devices cover the spectrum from partial support to total artificial hearts and from a temporary implant to a permanent feature. Ventricular assist pumps that are pneumatically powered are being used in the treatment of postoperative cardiac patients with profound left heart failure. An airdriven biventricular device is in trial use for end stage cardiomyopathy.
The problems that arise with these devices, such as high risk for infection, high risk for accidental detachment from the internal drive unit, and poor improvement to the quality of life imposed by pneumatically powered devices, makes their future acceptance doubtful as compared to the possibility of implantable, electrically powered assist devices. These systems, in trial and development stages, provide the basis for prolonged circulatory support.
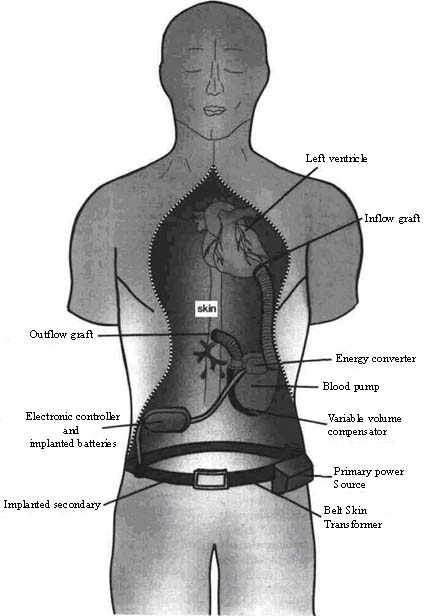
An electrically powered, mechanically activated, implantable left ventricular assist device (LVAD) that uses a unique, highly efficient, microprocessor-controlled solenoid energy converter coupled to a dual pusher-plate sac-type blood pump has been developed and is now in limited trial (Fig. 11.9). A newly designed belt skin transformer provides for transmission of primary power across the intact skin.
In clinical tests, a totally implantable, electrically powered LVAD has proven to be suitable for longterm use. Implant is via an outflow graft at the aorta below the diaphragm and an inflow graft at the apex of the left ventricle. The energy converter is situated on the top of the blood pump between the grafts. At this time, the device is not available for elective clinical use. Miniaturization of the electronic control system is in progress as are design refinements.
Indications for total artificial heart (TAH) include the patient with acute phase cardiac failure following cardiac surgery in cases where the surgery was not sufficient and recovery is not expected.8, 34 Preservation of the natural heart is possible. Other candidates are those with end stage cardiac disease due to cardiomyopathy or CAD. Pneumatically driven and mechanically driven artificial hearts are being studied.
|
|
Figure 11.9 Pneumatically powered artificial heart (Pennsylvania state). |
The Jarvik 7 TAH was first implanted in 1982. Although the ultimate goal of having the patient leave the hospital was not met, a great deal of information has been obtained. The Jarvik 7 TAH was able to improve renal performance and rapidly correct severe pulmonary edema. In addition, the cellular components of the blood were not damaged; there was no thrombus formation in the TAH; no infection occurred in the percutaneous leads; and good healing was noted at the skin-material interface. Further more, no gross or microscopic calcium deposits formed on the lining of the TAH, and the pumping components of the ventricles showed no evidence of wear or damage after 112 days of use.
Another type of pneumatic TAH is the Pennsylvania State University TAH (Fig. 11.8), consisting of two sac-type pumps, each one using a diaphragm to control sac motion.
The working premise of this model is (1) to increase left pump rate in response to decreased peripheral resistance (as reflected by a decrease in aortic pressure) or (2) to reduce left pump rate in response to vasoconstriction. The right pump will then speed up or slow down to maintain a relatively constant filling time of the left pump (left atrial pressure). There are also electric motor drive systems being developed.
Nursing ManagementPriorities for postoperative nursing care of a patient undergoing cardiopulmonary bypass for cardiac surgery are:
Nursing Diagnoses Most Frequently Associated with Patients Undergoing Cardiopulmonary Bypass for Cardiac Surgery
|
Temporary mechanical assist devices employing the principle of arterial counterpulsation have proven to be successful. Early cardiogenic shock has been reversed, coronary catheterization and angiography have been successfully carried out in the acutely ill patient with coronary insufficiency syndromes, and postoperative transplant patients and bypass grafting patients have been assisted in the weaning period of the cardiopulmonary bypass.
The principle of counterpulsation is to assist the heart in a natural series. The assist device, working in accordance with the ECG, results in a reduction of the systolic pressure and augmentation of the diastolic pressure, which in turn produces a markedly improved coronary perfusion. Total workload of the heart is reduced significantly (by 25%) with the intraaortic balloon pump (IABP). The IABP is the most effective device in use for assisted circulation (Fig. 11.10).
Several other devices have been considered, but the success rate does not approach that of the IABP.
IABPs are used primarily in cardiology and cardiac surgery but also can be of use in general surgery for high-risk patients. Cardiac failure is the main indication for the use of an IABP (Table 11.2). Better perfusion, better myocardial protection, and the use of catecholamines and nitrates in reducing afterload have decreased a great deal of the postoperative complications of cardiac failure. The new technique for percutaneous implantation of the balloon at the bedside has added to its use. The percutaneous intra-aortic balloon can be inserted in 5-10 minutes at the bedside. This technique could be extremely useful for assisting a heart in failure due to cardiomyopathy, particularly for the candidate awaiting transplant. The conventional insertion of an IABP requires a surgical incision.
| Table 11.1 Nursing Care Plan for the Patient Undergoing Cardiovascular Surgery | |||||
| Nursing Diagnosis | Assessment Data | Expected Outcome | Nursing Interventions | ||
| 1. | Fluid volume deficit related to loss of fluid during surgery, decreased fluid intake. | Subjective data: Patient states, "I am thirsty, I think I have a fever." Objective data: Patient is NPO Urine output is reduced Urine appears quite concentrated, dark color IV at keep-open rate only Weight loss recorded at 5 pounds since admission Mucous membranes are dry Tongue is coated Blood pressure decreased Tachycardia Peripheral venous filling time is greater than 5 sec Diminished skin turgor |
The patient will maintain fluid output equal to or greater than 2/3 of intake; will maintain a urine output of 30 ml/hr or greater. | 1. | Begin liquid diet as soon as possible. |
| 2. | Record intake and output. | ||||
| 3. | Monitor ECG for changes related to electrolyte imbalance. | ||||
| 4. | Monitor patient's skin color. | ||||
| 5. | Monitor IV fluids. | ||||
| 6. | Monitor and record hemodynamic parameters. | ||||
| 7. | Assess signs and symptoms of dehydration. | ||||
| 8. | Repeat assessments frequently for hydration, and correlate with hemodynamic parameters. | ||||
| 9. | Measure and record chest tube drainage. | ||||
| 10. | Record approximate insensible losses. | ||||
| 11. | Record character of drainage. | ||||
| 12. | Monitor all lab reports. | ||||
| 2. | Alteration in tissue perfusion: cardiopulmonary related to decreased capillary blood supply. | Subjective data: Patient complains of chest pain, difficulty breathing, numbness and tingling in extremities Objective data: Demeanor appears anxious Patient appears confused as to time and place Labored breathing with accessory muscles Diaphoretic Moist, cool skin Diminished peripheral pulses Diminished blood pressure |
The patient will demonstrate stable cardiopulmonary status, vital signs, adequate circulation. | 1. | Monitor for signs and symptoms of complications (e.g., tamponade, emboli, elevated blood pressure). |
| 2. | Assess for signs and symptoms of decreased perfusion (e.g., cold skin, diminished peripheral pulses). | ||||
| 3. | Assess sensorium. | ||||
| 4. | Monitor and record hemodynamic pressures. | ||||
| 5. | Monitor all systems until anesthesia effects are dissipated. | ||||
| 6. | Maintain patency of all lines and tubes. | ||||
| 7. | Record intake and output. | ||||
| 8. | Record amount and appearance of chest tube drainage. | ||||
| 9. | Maintain bed rest. | ||||
| 10. | Position for comfort. | ||||
| 11. | Record daily weights. | ||||
| 3. | Ineffective breathing pattern related to pain, hyperventilation, immobility. | Subjective data: Patient states, "I have trouble taking a breath. I feel lightheaded and dizzy." Objective data: Tachycardia Tachypnea Bounding pulse Rising blood pressure Face reveals anxiety Accessory muscles used in breathing Restless |
The patient will breath at an even and unlabored rate; will exhibit pink lips, nail beds; will show ABGs reflecting improved gas exchange. | 1. | Assess breath sounds; assess chest expansion. |
| 2. | Percuss lung fields. | ||||
| 3. | Evaluate pain as a contributing factor. | ||||
| 4. | Monitor and record color, character, and amount of chest tube drainage. | ||||
| 5. | Maintain patent chest tube. | ||||
| 6. | Position patient for ease of breathing. | ||||
| 4. | Potential for infection related to invasive procedures of surgery. | Subjective data: Patient states, "My incision hurts. I feel very warm. I am thirsty." Objective data: Elevated temperature Odorous drainage from operative area Inflamed incisional area Urine catheter in place Diminished breath sounds Tenderness at incision site IV maintained in place PA line |
The patient will be free from infection as evidenced by normal vital signs, clean incision, without purulent drainage or inflamed incisional area. | 1. | Maintain aseptic technique for all procedures involving possible infection sites (e.g., IV, insertions, wound dressing changes, urine catheter care and insertion, pulmonary artery line). |
| 2. | Change wound dressing daily; inspect and record appearance | ||||
| 3. | Get out of bed as soon as possible. | ||||
| 4. | Teach pulmonary toilet, cough, and deep breathing. | ||||
| 5. | Monitor temperature elevation. | ||||
| 6. | Report changes in sputum, urine, drainage. | ||||
| 7. | Turn patient frequently. | ||||
| 8. | Assess vital signs every 4 hours. | ||||
| 9. | Assess cerebral mentation. | ||||
| 5. | Impaired communication: verbal related to impaired ability to speak. |
Subjective data: Family reports patient is quite outspoken. Objective data: Endotracheal tube with assisted ventilation |
The patient will communicate needs with staff/family. | 1. | Teach pattern of blinks, nods, nonverbal communication methods. |
| 2. | Anticipate patient's needs. | ||||
| 3. | Explain nursing activities to patient before proceeding. | ||||
| 4. | Assist with removal of endotracheal tube. | ||||
| 6. | Alteration in comfort: pain related to surgical procedure | Subjective data: Patient states he or she is having trouble concentrating and is anxious about pain returning. Objective data: Guarded position Elevated blood pressure, pulse Tense body position Refuses to move about or get out of bed |
The patient will ask for nurse when pain begins: will verbalize relief of pain after medication. | 1. | Position for comfort, side-to-side, semi-Fowler's. |
| 2. | Place pillows and blankets for support. | ||||
| 3. | Use relaxation techniques when applicable (e.g., back rub, massage, skin rub). | ||||
| 4. | Administer analgesics by preferred route as ordered. | ||||
| 5. | Record effectiveness of medications. | ||||
| 6. | Evaluate possible signs and symptoms of infection. | ||||
| Table 11.2 Indications for Use of the IABP | |
| 1. | Postoperative failure while the patient is being weaned from bypass |
| 2. | Failure in the postoperative period |
| 3. | Cardiogenic shock with diminished function of the left ventricle |
| 4. | Impending infarction or extension |
| 5. | Uncontrolled tachycardia with Ml |
| 6. | A high-risk patient scheduled for coronary catheter or angiography |
| 7. | Cardiomyopathy following evaluation of cardiac status |
Many problems may lead to cardiac enlargement with increased left ventricular end diastolic volume. Congestive dilated cardiomyopathy is one etiology. An alternative to assisted circulation for these patients is the IABP. This can be used for the patient awaiting heart transplantation. The patient can then be mobile when he or she desires by disconnecting the pump. The pump is triggered by a normal ECG.
|
Figure 11.10 Placement of the IABP. |
A prophylactic dosage of an anticoagulation medication to prevent thrombus formation is added to the protocol.
This technique has been used successfully in two patients, and further trials are expected. Another possible use of the implanted IABP may be to relieve strain on the heart when chronic inflammatory myocardial disease is present.
Nursing ManagementPriorities for nursing care of a patient undergoing IABP are:
Nursing Diagnoses Most Frequently Associated with IABP
|
Although this is not a surgical technique, it is a relatively new method for treating coronary artery disease and is associated with bypass surgery. (Patients in whom the balloon angioplasty is not successful are usually sent to surgery immediately for CABG surgery). PCTA, which is being used with increasing frequency, is a procedure for dilating an occluded coronary artery by using a balloon catheter. Estimates disagree, but approximately 10% of patients undergoing CABG surgery are candidates for PTCA. The patient selection process is very specific. The best candidate is one who (1) presents with severe incapacitating symptoms of angina; (2) would be a candidate for a CABG; (3) has a single lesion in the left proximal anterior descending, left circumflex, or right coronary artery; and (4) has no calcification in the lesion.6, 16
PTCA is accomplished with local anesthesia. The approach is usually through the femoral area, but the brachial area may also be used. The procedure forcefully dilates an occluded artery by the use of balloon inflation. Dilatation is usually successful with multiple balloon inflations.
Controversy about this procedure centers around postmortem evidence that reports cracks in atheromatous plaque and the intimal lining of the arteries. The surface then becomes vulnerable to platelet aggregation and thrombus formation. The final decision concerning the long-term benefits of the procedure is still controversial.
Another procedure related to PTCA involves intracoronary artery infusion of streptokinase. Streptokinase is an enzyme that triggers a chemical action, causing fibrinolysis. This procedure may be used in patients with new onset of acute MI. The infusion must begin within 4 hours of the onset of infarction symptoms. Prompt lysis of the clot is the objective of this treatment. Selection of candidates for PTCR varies among institutions. Contraindications for the procedure are recent major surgery, a cerebral vascular accident, recent CPR, endocarditis, significant valve disease, or risk of hemorrhage. The procedure introduces a catheter into the occluded artery with a carefully monitored drop of streptokinase. Usually a 20,000 unit streptokinase bolus begins the procedure, followed with a constant infusion of 2000 units per minute. Protocols vary. Coronary angiography is performed repeatedly to measure results. The infusion is continued until the thrombus is lysed or until 60-90 minutes of infused medication has been administered. Reperfusion occurs rapidly; however, many patients show some evidence of myocardial necrosis, evidenced by a rise in the MB band of the CPK and Q waves evident on ECG. The successful PTCR treatment is often followed by CABG because of the tendency for further occlusive lesions. Practitioners report a success rate of 60%-85% in the reestablishment of blood flow. Long-term success rates, however, will require further study.
Nursing ManagementPriorities for nursing care of a patient undergoing a PTCA or PTCR are:
Nursing Diagnoses Most Frequently Associated with PTCA or PTCR
|
Heart block is the most frequent underlying cause demanding a pacemaker. A pacemaker insertion refers to a mechanical device consisting of a pulse generator and an electrode that will initiate an artificial electrical stimulus for myocardial contraction.19 The pulse generator is a battery-powered energy source. The wire delivers the electronic stimulus to a contact point in the myocardium. The sole purpose is to send an electrical impulse from the power source to the atrium and / or the ventricle to stimulate myocardial contraction. Conduction defects and heart blocks are the most frequent underlying causes demanding a pacemaker. When the heart's own conduction system is not functioning normally, varying degrees of block may occur. Pacemakers may additionally be used prophylactically during surgery for persistent block.
If heart block is the problem, the electrode is placed in the ventricle to ensure stimulus beyond the block. The electrode may be placed in the atrium to assist the sinoatrial (SA) node and to suppress ectopic impulses unresponsive to medication. The electrodes for permanent pacing are placed in one of two methods: transthoracic or transvenous. Transthoracic pacing is usually used only for emergency pacing. This involves threading the pacing wire through a percutaneous intracardiac needle or directly through the chest wall via an introducer into the myocardium. The needle or introducer is removed, leaving the electrode in place. When open chest surgery is in progress, a transthoracic epicardial placement may be used. Pacemaker insertion is a procedure that is usually performed under local anesthesia.
The most common procedure for pacemaker implantation is the transvenous endocardial approach. This involves the threading of an electrode or electrodes through a vein into the right atrium or right ventricle. A 3- to 4-inch incision into the deltopectoral groove on the chosen side is made to create a pouch for the insertion. The subclavian or cephalic vein is selected for threading the electrode. The distal end of the electrode is inserted. Side preference is usually decided by the patient. Tennis players, golfers, or left-handed writers may favor one side or the other. The most frequent entry site chosen by surgeons for the electrode lead wire is the right or left cephalic vein. The wire is then directed via fluoroscope into the heart. After proper placement and testing of the electrode, the pulse generator is inserted in the pouch. The pulse generator is powered by lithium iodide electrochemical cells, which are safe, reliable, and long-lasting. Nuclear generators are also used.
At present, there are three pacing modes designed to supply a steady impulse to trigger the heart's pumping action: fixed-rate pacemakers, demand pacemakers, and synchronous pacemakers.
Fixed-rate pacemakers are the early modes. They are also known as asynchronous models. This type delivers an impulse at a preset fixed rate independent of the heart's own conduction activity. It does not have the capacity to sense the patient's own rhythm. The one advantage of this mode is its simple circuitry, which reduces the chance of pacemaker failure. The fixed-rate pacemaker is used infrequently today because more advanced models are on the market.
Demand pacemakers are used to pace the atria or ventricles. This mode is also referred to as the QRS complex-inhibiting mode. The pulse generator has a sensing device. If the patient's natural rate drops below a preset rate, the pacemaker delivers an electrical stimulus. The pacemaker fires only when needed. The demand pacemakers are programmable or nonprogrammable. The nonprogrammable type has an impulse rate and voltage level set at manufacture and is not alterable. The usual rate is 72 bpm and 5 milliperes. The programmable mode, used more frequently today, responds to an external programming unit that allows the physician to set rate and voltage at the time of implant or later, if necessary. Demand pacemakers used to pace the ventricle are of three types: (1) R wave-inhibiting, in which the sensing mechanism senses ventricular depolarization and does not fire unless the preset escape period has passed without the occurrence of a depolarization. This is a preset unit and will fire if the inhibiting impulse does not occur. (2) The R wave-triggered mode is set to deliver an impulse during the patient's own QRS complex. Depolarization of the patient's ventricle triggers this mode to fire. Problems with this mode occur when evaluating the QRS complex because the pacemaker spike distorts the complex. (3) The hysteresis pacemaker is a demand pacer with a built-in delaying factor. The escape interval is longer than the pacing interval. The pulse generator may be set for 70 bpm, but the pacer will not fire until an interval of a 10-beat margin occurs. This pacemaker can sense and pace at different intervals. If the patient's rate is below 71 bpm, the pacemaker can start at 85 bpm or whatever rate is chosen, not just at the 72 bpm rate. The advantage to this delay pacer is that it allows for normal heart slowing, such as in sleep or at rest. Patients with bradycardias may use this mode to advantage, but the patient with frequent premature ventricular contracts is at a disadvantage because the longer space between beats can produce ineffective ventricular cycles, reducing cardiac output. Demand pacemakers are also used to pace the atrium. Two types are in use: (1) atrial P wave-inhibiting units have the sensing and pacing electrodes implanted in the atrium. This mode fires after a predetermined time frame in response to failure of the natural atrial depolarization. The atrial demand pacemaker can only function with an intact AV conduction system. (2) P wave-triggered atrial pacing also means that the pacing and sensing electrodes are embedded in the atrium. This mode fires with the P wave and will fire independently when the sinus node fails to fire within a predetermined time frame.
Synchronous pacemakers are a demand mode pacemaker of a different type. This mode, termed the AV synchronous, has two electrodes, a sensing electrode in the atrium, and a stimulating electrode in the ventricle for ventricular stimulation. The sensing electrode in the atrium recognizes the patient's atrial depolarization, holds for a preset interval to match the PR interval, then triggers the ventricular pace-maker. This synchronized activity relates to the normal cardiac cycle. A safety feature allows the ventricle to fire independently from the atrium if the atrial rate becomes excessive. This is a demand device, so the ventricular pacemaker will fire if an atrial impulse does not appear after a given interval.
Research is now in progress for a pacemaker with a physiologic sensing mode. This type would alter heart rate by sensing electrolyte changes, oxygen and carbon dioxide blood levels, and other hemodynamic parameters. These pacemakers are still in the developmental stages.
The Inter-Society Commission for Heart Disease Resources discusses pacemakers in terms of letters or pacemaker identification codes (Table 11.3). Pacing systems have been classified using a universal code. The first letter represents the chamber paced, the second letter, the chamber sensed, the third letter, the pacing mode; if used, the fourth letter, programma-bility; and the fifth letter, the antitachycardia functions. The three letter code is most frequently used.
| Table 11.3 Pacemaker Code | |
| The Inter-Society Commission for Heart Disease
Resources discusses pacemakers in terms of letters. The Letters |
|
| 1. | Chamber paced V - ventricle A - atrium D - both (dual chamber) |
| 2. | Chamber sensed V - ventricle A - atrium D - both 0 - not applicable |
| 3. | Mode of response I - inhibited T - triggered D - inhibited and triggered 0 - not applicable |
| 4. | Programmability P - programmable rate and/or output M - multiprogrammable, mode, AV delay, sensitivity, hysteresis 0 - None |
Programmability is the feature of the pacemaker by which the electronically controlled performance can be altered noninvasively. All of the new models of implanted pacemakers are multiprogrammable. The pacer is programmed with the use of an external programmer to transmit preselected codes to the implanted pulse generator. Radio waves or a pulsed electromagnetic field carry the message. New models now carry added protection against accidental repro-gramming by requiring an electronic password before an alteration in the code occurs. The ECG tracing confirms reprogramming. Features that may require changes are output, rate, and escape rate. The voltage, current, and pulse duration make up the pulse generator output. Rate is the interval between consecutive atrial or ventricular-paced stimulation. The setting is programmable and can be increased or decreased. It may be necessary to increase the rate to override tachycardia or to compensate increased metabolic needs. Decreased rate may be necessary to alleviate angina or to reduce discomfort experienced by patients with new pacers who cannot tolerate the paced rhythm. Sensitivity is the system's ability to sense the patient's intrinsic signal and to react to control the firing of the pacemaker. The sensing circuit recognizes an R wave or a P wave by its amplitude and slew rate, the change of voltage amplitude with time. The sensing circuit differentiates between the QRS and the T wave by recognition of the slew rate.
Escape rate is the interval between the last-sensed beat and the first pacemaker beat that follows. When the escape rate is longer than the programmed interval, it is termed hysteresis. Pacing does not begin until the rate falls under 60 bpm, even though the pacemaker may be programmed to pace at 72 pulses per minute. This time lapse gives the patient a better chance for conducted beats.
The commonly used single chamber pacemakers are VVI (Table 11.3) units, which have programmable output, rate, and sensitivity. Pacing and sensing are limited to the ventricle. The intrinsic activity of the ventricle inhibits output of the pulse generator.
The commonly used dual chamber pacemakers are the DVI and DDD units. The DVI mode paces the atrium and the ventricle (dual); sensing is only in the ventricle. The pacer is inhibited by the intrinsic activity of the ventricle.
In the DDD mode, both pacing and sensing occur in the atrium and ventricle; atrial or ventricular output put is inhibited by sensed activity of either chamber; and ventricular output is triggered by sensed atrial activity.
Symptomatic bradycardia is the most common problem requiring pacemaker insertion. Some other indicators for permanent pacing19, 28 are:
The choice of pacemaker to accommodate the problem is emphasized. For the patient with chronic atrial fibrillation, for the elderly inactive patient, or for the patient in whom the pacemaker is to be a standby device, a VVI pacemaker should be the choice. Dual chamber pacing is more applicable for the patient with heart block and an intact sinus mechanism because this node allows the ventricular rate to increase with the sinus rate. Generally, the implantation is done under local anesthesia in the operating room. Cephalosporin antibiotic is usually administered before and for up to 24 hours following the procedure.
Some of the possible complications of implanted pacemakers are:
The emergency use of an external cardiac pacemaker has proven to be effective in treating some patients with symptomatic bradycardias and some cases of asystole. It has proven life saving when applied to patients with a responsive myocardium. The external pacing device is capable of functioning in a fixed-rate or demand mode. The pacemaker in use at this time is a Zoll Noninvasive Temporary Pacemaker, manufactured by the ZMI Corporation (Fig. 11.11). Application of two electrodes in the usual manner to the chest wall achieves the pacing. The first is attached at the cardiac apex and the second on the back in the left subscapular area. An electrocardi-ograph monitor sends a signal to the pacemaker, permitting sensing of the patient's intrinsic rhythm. The pacing stimulus travels through the electrodes. The rate can be varied from 0 to 180 bpm. The pacemaker functions in the demand mode. The pacer activity is monitored via an oscilloscope. The pacer senses cardiac repolarization (the T waves) following the pacemaker stimulation. When the ECG electrodes are disconnected, the pacer functions in a fixed-rate mode. External pacing has several advantages over temporary transvenous pacing in some clinical situations. Familiarity with the device is the only requirement for use. It can be applied quickly in an emergency situation. Use of the external pacer allows time for careful insertion of a transvenous pacer. In the patient undergoing permanent pacemaker implant, the external pacer can be used to pace the heart if asystole occurs during the procedure. Another reason for its use is to reduce the number of temporary catheter electrodes inserted prophylactically in patients at risk for high degree conduction defects. The number of complications (e.g., sepsis, pulmonary embolism, arrhythmias) is also reduced when the external pacer is used.
|
|
|
Figure 11.11 The Zoll NTP. |
Nursing ManagementPriorities for nursing care of a patient with a pacemaker are:
Nursing Diagnoses Most Frequently Associated with a Patient with a Pacemaker
|