|
|
Table 2.1 Family History Chart |
| Contents | Previous | Next |
An understanding of the anatomy is necessary to take an accurate history and do a complete examination of the heart. Diagnosis is often based on the history. Informed clinical judgments can be made on the basic information from the chief complaint, the medical history, and the present illness. The first step in a nursing assessment of the heart is data collection. The nurse takes a patient's medical history, beginning with questions about symptoms: chest pain; cough; shortness of breath; breathing problems while lying down or at night; weight changes; swelling of ankles, hands, or legs; fatigue; or dizziness or syncope.
Chest pain is a frequent complaint. Ask the patient to describe the pain by onset, severity, location, duration, and radiation. Ask about activities that produce, aggravate, or relieve the pain. Question the patient about medications (both prescribed and overthe-counter) that are used to obtain relief. Coronary pain is not always located in the anterior chest. It is not uncommon for cardiac pain to originate in the arms, jaw, epigastrium, neck, or shoulder. Patients sometimes describe a feeling of heaviness in the chest or in the arm. It is a rare patient who can point to one area of localized pain. A clenched fist over the chest, referred to as a positive Levine's sign, is frequently the demonstrated description of the pain.
Patients with angina may describe tightness, heaviness, and pressure in the chest when asked about pain. The infarction patient uses descriptions such as crushing, choking, viselike pain. The pain of pericarditis may be identified by sharp pain, intensified by deep breathing, movement, or lying down and relieved by sitting up and breathing shallowly.4 A characteristic that is associated with pericarditis but frequently is not recognized is a pain that radiates to the left shoulder.
Chest pain may be the chief complaint in patients with problems not of a cardiac origin. Gastrointestinal diseases such as ulcer, esophagitis, hiatal hernia, cholecystitis, and pancreatitis are examples of such problems that may resemble heart distress. A complete history may help to differentiate cardiac disease from chest pain of other origins. A dry cough is frequently the first symptom of a failing heart. Ask the patient to describe the cough. Is it productive? Ask when the cough became evident.
Dyspnea may be the chief complaint. Breathing difficulties can be linked with heart disease. Ask about the onset of shortness of breath, nocturnal breathing problems, and the number of pillows required for sleep. Ask the patient to describe breathing discomfort on exertion. Determine if this is a new development or one that has developed slowly over time.
Fatigue is an early symptom of heart disease.5 Check fatigue levels and ask about exercise, activities of daily living, and changes in the levels of performance. Ask if the patient is able to climb stairs or walk across the parking lot or around the block. Do routine home chores produce exhaustion? The assessment should determine the activity levels that produce dyspnea and determine if a change has occurred in these levels.
Explore any statements about dizziness or syncope. Have the patient describe the depth of the problem. Does the patient experience a faint feeling, temporary confusion, vertigo, or an inability to stand? Is it lightheadedness or complete blackout? If it is a complete blackout, how long does it last? The temporary loss of consciousness is referred to as syncope. Cardiovascular disease is sometimes associated with TIAs, or transient ischemic attacks. Differential diagnosis is again important to determine if this is cardiovascular or cerebrovascular in origin. Ask the patient about the frequency of the fainting episodes and when and where they happen. Ask about precipitating factors, such as the relationship of onset to events such as exercising; coughing; voiding; putting on a tie; turning the head to comb hair; or experiencing emotional problems, fear or anxiety, or neck pressure. Have the patient describe any discomfort preceding the attack, such as palpitations, ringing in the ear, nausea, numbness, slurred speech, or headache. Check the patient's present medication regimen for drugs that may cause hypotension.
Edema with weight gain may cause the patient to seek medical attention. Descriptors usually include swelling in hands and feet or puffiness all over, particularly after sitting for a period of time. The edema produced by fluid extravasation from intravascular to extravascular spaces becomes more evident during the wakeful hours. Patients often describe ankle swelling as being progressive in nature, so that by evening it may be difficult to wear shoes. Patients also describe being awakened frequently at night to void, the diuretic effect of the retained fluid.
Next, obtain a more detailed description of the chief complaint. Ask the patient to describe the development of the problem. Ask when the problem began and continue to elicit information encompassing the progression to this point. Have the patient describe the problem from time and manner of onset; changes;
discomfort either increasing or decreasing in severity, frequency, and duration; location; and any factors that affect the problem, such as time of day and events preceding onset. Ask about alleviation with medication, rest, or discontinuation of an activity. The chief complaint may be something other than a blackout or a pain. The patient may become aware of subtle or not so subtle changes, such as weight gain, fatigue, edema, or palpitations. Have the patient describe the changes. Ask if other symptoms accompany the chief complaint. The patient may describe a diagnostic syndrome. It is important to assess whether the chief complaint is always a part of other symptoms or if it is a rare association.
Medical history includes the presence of allergies (food and drug), personal habits, injuries or accidents, childhood diseases, past illnesses, and a social history. Medications taken on a regular basis should be included in the history, as well as recent travel and military history, if it is applicable. A detailed past history may provide a basis for differentiating between the present chief complaint and a problem of the past. Factors predisposing specific problems may come to light.
Allergic reactions should be explored. Cardiac patients are frequently taking a variety of medications, prescribed and over-the-counter. Allergy to emergency medications should be explored, as well as allergy to any antibiotic medication. Ask about food allergies or transfusion problems in earlier circumstances.
Eating, smoking, drug, and alcohol histories are important. Questions about smoking history relate directly to cardiovascular problems, as do questions about food, eating habits, and weight problems. Smoking should be recorded in pack years—packs smoked per day multiplied by the number of years the patient has been a smoker. Example: If Mr. Smith smokes 2 packs per day for 20 years, he is recorded as a 40-pack-year smoker.
Injury or accident history should include information about blows to the chest, gunshot or stab wounds, prolonged bleeding injury, bum injury that may have impaired circulation, and automobile accidents. Question the patient about any electrical accident or any injury that led to medical intervention.
Childhood diseases and past illnesses are explored to discover streptococcal infections, viral infections, and rheumatic fever. Previous chest disorders, chest pain, or history of angina or previous myocardial infarction should be included. Elevated or lowered blood pressure with medication regimen should be noted. Information about bypass surgery, valvular or aneurysm repairs or venous or arterial procedures may relate to the present problem.
A social history includes the patient's occupation, marital status, family, and life-style. An example of the typical daily diet should be elicited with the alcohol intake. Hobbies and exercise regimens can be noted with personal data.
Data regarding over-the-counter products used frequently, such as aspirin, cold medications, and antacids, should be included.
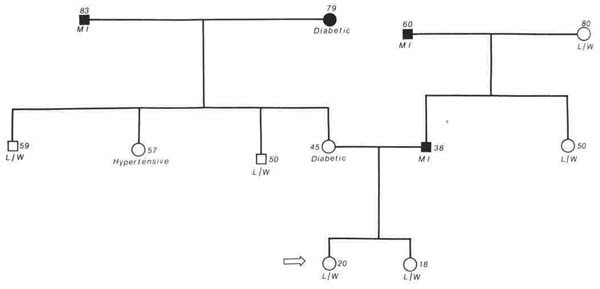
Hereditary and familial predisposition is an important element in a patient assessment. The immediate family—grandparents, parents, siblings, and children—rather than relatives through marriage are included.
The age, sex, and health status of family members may be recorded as shown in Table 2.1. Deceased members are recorded with cause of death, if it is known.
|
|
Table 2.1 Family History Chart |
Following data collection, the physical examination is the next step in assessment. The physical examination proceeds in an organized manner through the cardinal parts: inspection, palpitation, and auscultation.
|
|
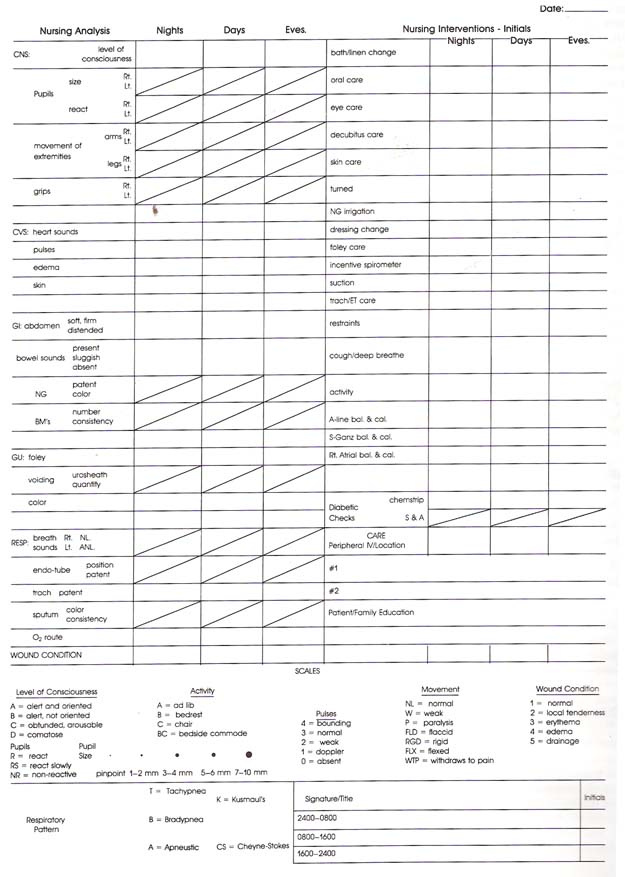
Table 2.2 Nursing Analysis and Intervention for the Cardiac Patient |
The patient is disrobed to the waist and examined in supine, left lateral, and sitting positions. A sphygmomanometer, a stethoscope with bell and diaphragm, and a sweep second-hand watch are the necessary equipment to perform a cardiovascular exam. The normal heart lies in an oblique position behind the sternum, with the largest section to the left of the midline. The left border extends from the second to the fifth intercostal space.12 This oblique position places the right atrium and right ventricle as the primary chambers anteriorly, which leaves a very narrow area for the left ventricle at the left cardiac border.
Examination begins with inspection for general appearance. Chest contour is observed for stemal depression, symmetry, localized bulges, and abnormal pulsations. Slight asymmetry is not pathologic. Locate the apex of the heart and visually note the point of maximal intensity (PM1). The PMI is usually found in the fifth intercostal space (ICS) on the left at the midclavicular line. In the enlarged heart, the PMI will shift outward and downward. Pericardial effusion may also cause a bulge at the PMI.
Observe the neck veins for pulsations and level of distention as an estimate of venous pressure.4, 7 Neck vein examination includes observation of venous wave forms, auscultation for cervical venous hums, and estimation of venous pressure. The internal jugular vein is frequently referred to as the manometer of right atrial pressure because of its direct connection with the vena cava, which leads directly to the right atrium. A continuous pathway is in place, unhampered by valves. This allows pressure changes in the right atrium to travel this pathway and be detected in the internal jugular vein. When pressure in the right atrium is elevated, venous pressure rises throughout the system, and the veins become distended due to the engorgement. Veins close to the heart reflect greater distention. In the internal jugular vein, as pressure rises, the distention moves from the base of the neck toward the earlobes. Distention causes visible venous pulsations, and the pressure in the right atrium can be estimated by measuring the level reached by the pulsations.
Observations are made first with the patient in a supine position and then with the patient elevated to a 45° angle. Neck veins should normally collapse when the head is elevated.4, 7, 17 Hands and feet are inspected for color, hair distribution, pulsations, or venous bulging. Nails are inspected for color, shape, clubbing, or thickening. Changes may indicate an oxygenation problem. Extremities are inspected for skin color, hair distribution, texture, edema, or any unusual appearance.
|
|
|
Figure 2.1 Palpation of the heart |
Palpation of the heart begins with the patient in a supine position (Fig. 2.1). Some abnormal movement is not visible but may be found with palpation. The precordium is examined at the right and left sternal borders, the point of maximal intensity, and the pulmonic and aortic areas.20 Fingertips and palmar and ulner hand surfaces are used for palpation. The apical impulse might not be felt when the patient is supine. With the patient leaning forward in a sitting position, the pulse is more readily felt. Vibrations and pulsations should be noted. Vibrations (also referred to as thrills) may indicate turbulent blood flow. The suprasternal notch, the second right interspace (aortic), the second left interspace (pulmonic), and the left heart border are the primary areas to palpate for thrills. When a thrill is palpated, it is important to determine if it is systolic or diastolic. Simultaneous palpation of the carotid pulse and the thrill determines the place in the cardiac cycle. The carotid pulse coincides with the closing of the mitral and tricuspid valves. While a thrill is palpated, it is important to place the stethoscope over the area to determine if a sound is heard. The sound is referred to as a bruit.
Palpate all arterial pulses, recording rate, rhythm, and amplitude (1+—greatly diminished, 2+—slightly diminished, 3+—normal, 4+—bounding). Bilateral comparison of pulses on each side is recorded.
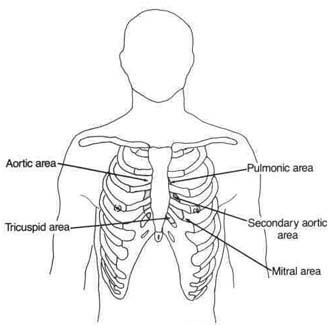
Aortic, pulmonic, mitral, tricuspid, and left sternal border are the five auscultatory sites for heart sounds.20 These sounds are produced by valve closure, with the sound projected in the direction of blood flow. Closure of the mitral and tricuspid valves produces the first heart sound (S1). It is loudest at the apex or mitral area of the heart. This is usually a single sound, described as a "lubb" sound. This S1 is synchronous with the carotid pulse. The period following the first heart sound is called systole. The ventricles contract at this time to pump blood.
The second heart sound (S2) is created by closure of the aortic and pulmonic valves and is best heard at the base of the heart. In this area, S2 is louder than S1 and is composed mostly of aortic valve closure. The pulmonic sound occurs slightly later than aortic closure vibration and can be heard over the pulmonic valve in the second left intercostal space.20 This normal physiologic splitting results from right ventricular systolic ejection time being delayed by a fraction of a second. It is best heard during inspiration. Wide splitting of S2 indicates an abnormality such as a conduction defect, stenosis, or atrial septal defect.S2 is usually described as the "dupp" of the "lubb-dupp" sound.
|
|
|
Figure 2.2 Areas for auscultation of heart sounds |
The third heart sound (S3) normally may be heard in children and young adults but disappears by the late twenties. In the older adult, it suggests cardiac impairment such as congestive failure. It is a lowpitched sound best heard in early diastole at the apex with the bell of the stethoscope.S3 is thought to result from vibrations produced by rapid filling of the already overloaded ventricles.S3 is referred to frequently as a 'ventricular gallop and is described as Kentucky S1, S2, S3.20
The fourth heart sound (S4) is also best heard with the bell of the stethoscope. It is heard in late diastole just before or combined with S1. This fourth heart sound is not a normal heart sound and is thought to be caused by late ventricular filling resulting from forceful contraction of an enlarged atrium. S4 is best heard at the apex and is described as Tennessee S4, S1, S2.
Murmurs are described as audible sounds produced in the heart and great vessels by turbulent blood flow.20 The cause of murmurs is often debated, but three influencing factors have been recognized:
Murmurs are described with respect to anatomic location, timing (systolic or diastolic), quality, radiation, and loudness. Murmurs are graded:
Grade I — very soft, barely audible
Grade II — faintest audible
Grade III — moderately intense
Grade IV — loud but may be difficult to distinguish
Grade V — loud but audible with the stethoscope
Grade VI — audible without the stethoscope
A systolic murmur occurs betweenS1 and S2 and may be ejection or regurgitant. Mitral regurgitation or mitral insufficiency heard at the apex with a soft swish sound is one example. Aortic stenosis located at the aorta has a harsh sound. Diastolic murmurs occur betweenS2 and S1 and result from either filling or regurgitation. Examples are mitral stenosis, heard as a low-pitched rumbling sound, and aortic or pulmonic insufficiency, heard at the base as a highpitched blowing sound.
Pericardial friction rubs result from inflammation of the pericardial sac. The sound is made by inflamed layers of the pericardium sliding over each other. It may be heard as a high-pitched scratchy sound.
Cardiac valves normally do not make sounds on opening. If stenosis of the semilunar valves is present, a sound early in systole may be heard; this is called an ejection click. It is a loud, clear sound heard best during exhalation. A sitting position may enhance its loudness. Ejection clicks may be caused by sudden opening of the aortic and pulmonic valves.
During diastole, an opening snap — a sharp, high-pitched sound — may be heard. Normally, the opening of the mitral valve is not heard. A highpitched opening snap indicates mitral or tricuspid stenosis. Extra heart sounds are frequently difficult to hear and classify. A great deal of cardiac assessment skill is necessary to interpret their significance.