|
|
|
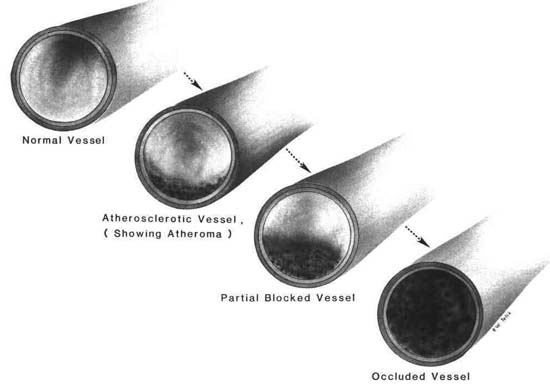
Figure 3.1 Progressive atherosclerosis |
| Contents | Previous | Next |
Coronary artery disease (CAD) is not one delineated dysfunction. CAD should be thought of on a continuum, moving from the etiologic factors of emboli and thrombi, to arteriosclerosis, the most common cause, leading to severe dysfunctions.
Arteriosclerosis, a term meaning hardening of the arteries and describing several artery degenerative diseases, can occur in any artery. The coronary arteries, the aorta and its main branches, are particularly at risk. Areas of high-pressure blood flow, directional changes, and bifurcation points put special stress on the intimal layer of the artery wall. Arteriosclerosis attacks large- and medium-sized arteries to a grea.er degree than it attacks smaller ones. Lesions do not appear close to the arterioles.
Three layers make up the artery wall: the inner lining, called the tunica intima; the tunica media; and the outer layer, or tunica adventitia. It is the intimal layer of the arterial wall that is primarily involved with atherosclerosis.
Atherosclerosis develops over a long period (Fig. 3.1). The lesion begins with fatty plaque formations in the tunica intima. The plaques are made up of plasma lipids—cholesterol, triglycerides, phospholipids, and fatty acids. These plaques cause obstruction, with narrowing of the lumen of the artery. The plaques irritate the artery wall, causing inflammation and scar formation; a fibrous plaque is produced. As the process continues, calcification occurs and calcium deposits are added to the plaques. The hardening of the artery wall with these fibrous and calcium deposits over the lipid plaque produces the lay term, "hardening of the arteries." A calcified lesion of atherosclerotic disease can result in a greatly reduced internal diameter, restricting blood flow and leading to ischemia, infarct, and necrosis. The irregular surface of the lesion may eventually lead to thrombi formation.58
|
|
|
Figure 3.1 Progressive atherosclerosis |
Although the exact etiology of coronary atherosclerosis with resultant heart disease is multifaceted and not completely understood, factors that influence coronary atherosclerosis to some degree have been identified. These include:
The major indication of atherosclerotic impairment of myocardial perfusion is chest pain. Signs and symptoms are not present unless myocardial oxygen supply is reduced by narrowing or obstruction to the point of ischemia. The pain is related to the degree of obstruction and the number of involved coronary arteries.
Therapeutic intervention is dependent on progression of the obstruction. Counseling to change behaviors such as smoking, diet, and life-style is a valuable intervention. As the disease progresses, however, surgical procedures are frequently the interventions.
Angina pectoris literally means pain in the chest. Angina should be viewed as a symptom on a continuum, rather than as a disease entity. The coronary arteries are responsible for oxygen delivery to the myocardium. Seventy-five percent of the oxygen carried by the coronary arteries is extracted in a normal resting state. When the heart must work harder, there is increased demand for oxygen. The demand cannot be met by further extraction because the system has little reserve. An increase in coronary blood flow is required. The new demand may be for four times the normal flow. When a discrepancy between oxygen demand and the ability of coronary arteries to supply occurs, angina is the result.
Angina has two forms—stable and unstable. Stable angina refers to a condition that has followed an unchanging pattern for at least 60 days. The onset, duration, and degree of discomfort have remained the same. The discomfort may be mild or disabling but usually will be relieved with rest or nitroglycerine within 3-5 minutes.
Unstable angina is the more ominous type. This type of angina is progressive,51, 54 with changes in precipitating events, duration, frequency, and severity. Unstable angina is identified by unpredictability of attacks and includes recent onset angina. It can occur at any time, when the patient is awake or during sleep. One variant type of unstable angina, known as vasospasm, is Prinzmetal's angina. The patient experiences chest pain while at rest. The periods of chest pain lengthen. Diagnosis of this variant type of angina is with electrocardiogram (ECG). Normally, the ST segment is isoelectric; it follows the baseline of the ECG. When the pain is present, ST segment elevation is present, with an upright or inverted T wave, reflecting myocardial ischemia. The ST segment returns to normal when the pain dissipates (Section One, Chapter 1). Depression of the ST segment of more than 1 mm is usually seen in patients with angina.
Other ECG changes may occur with the ST changes reflected by coronary artery spasm. The right coronary artery usually supplies the AV node. Spasm in this artery may produce a heart block for the duration of the spasm. Irregular ventricular beats, such as ventricular tachycardia, premature ventricular beats, or ventricular'fibrillation, may complicate a spasm in the left anterior descending artery.
The pain of angina is thought to result from a lack of oxygen (anoxia) in the myocardium, with a resultant rise in carbon dioxide and production of lactic acid. Spasm of coronary arteries and partial obstruction are also possible causes for reduced blood flow.
There are several theories about the cause of coronary artery spasm, but the exact etiology is not understood. However, several factors may contribute to this problem: atheromatous plaque deposits in the lumen of the artery, which increase the intensity of spasm; hemorrhage into medial layers of the artery, which creates an irritation leading to spasm; vasoconstriction resulting from hyperventilation with decreased hydrogen ion concentration and elevated calcium ion levels; or catecholamine elevation with a resultant rise in sympathetic tone (alpha adrenergic stimulation), which can increase the risk of spasm in the coronary arteries.
The etiology of variant angina may be coronary artery spasm alone or in combination with atherosclerotic disease. If little atheromatous plaque is seen on angiography, a testing drug, ergonovine, may be injected to induce coronary spasm for diagnosis. Prolonged anginal attacks with myocardial ischemia may eventually progress to myocardial infarction.
Chest pain is the descriptor when angina occurs. The pain is classic, described as substernal or over the left precordium. The patient will say it is a squeezing, viselike pressure, with a burning sensation.
The pain is frequently brought on by exertion, stress, or cold, or it may occur after a large meal. The pain may radiate to the neck, left arm and shoulder, and as far as the left hand. All of the fingers may be involved. Occasionally, the right shoulder, arm, and hand are affected. Pain radiation may include other areas, such as the lower jaw, larynx, or trachea, and occasionally, epigastric pain is noted.
Angina pain is characterized by a gradual increase and decrease in intensity.
Therapeutic intervention is dependent on the characteristics and the pattern of occurrence of the disease. Medical treatment for classic angina is directed toward decreasing oxygen demand. Interventions include rest, nitrates, and beta blocking medications. Coronary artery spasm with reduced artery lumen requires vasodilatation with nitrates and calcium channel blocking agents.
Sublingual nitroglycerin (NTG) is the drug of choice for the acute treatment of angina (Section Five). The major effect of NTG is a decrease in peripheral resistance, with increased venous capacity. The coronary arteries are also dilated. Sublingual NTG is a drug of short duration. Pain relief is prompt. The beta adrenergic blocking agents, with the capacity to decrease myocardial contractility, heart rate, and cardiac workload, thereby decreasing oxygen demand, are used in the treatment of classic angina. Propranolol and metoprolol are examples of these medications.
The calcium channel blocking agent, nifedipine, has proven effective in the relief of coronary artery spasm.
Patients with poor response to medical management, and those with unstable angina pectoris are
candidates for coronary angiography and possible coronary artery bypass graft surgery.
Nursing ManagementPriorities for nursing care of a patient with angina pectoris are:
Nursing Diagnoses Most Frequently Associated with Angina Pectoris
|
Death of heart muscle or infarction occurs when the blood supply to the myocardium is interrupted for a period long enough to cause necrosis, about 20 minutes. The infarcted area is surrounded by an area of injury and then an area of hypoxia.
Myocardial infarcts usually occur in the left ventricle. A transmural infarction means that the full thickness of the myocardial wall is involved. Infarcts involving only the inner portion of the myocardium are called subendocardial infarcts. It is theorized that infarcts usually begin as subendocardial and progress to transmural.14
Severe myocardial ischemia produces a reduction in coronary arterial blood flow.2 With the onset of cellular ischemia, metabolic changes occur; there is a shift from aerobic to anaerobic metabolism, and lactic acid formation occurs. If the condition persists for a short period, the myocardial injury is reversible. The exact timing is not established, but about 20 minutes is considered maximum duration for the injury to be reversible. It is believed that when glycogen is depleted, cellular edema is present, the mitochondria swells, and myofibrillar relaxation occurs. The injury to the myocardium is not reversible, and there is cell death. In association with leakage from the cells of enzymes (CPK-MB), a colorless or pale section appears in the necrotic myocardial area. Gross pathologic changes due to the infarction become prominent at 18-24 hours postinfarct. The infarcted area appears cyanotic and swollen. Over the course of time, a shrunken white scar develops, progressing to endocardial thickening in the infarcted area.
The etiology of AMI can be an isolated problem or a combination of problems, such as further occlusion of a coronary artery already narrowed by atherosclerotic plaque, the result of a thrombotic clot; prolonged spasm of the artery; reduced blood flow to a section of myocardium; or hemorrhage into an already atherosclerosed arterial wall. Any factor that reduces blood flow and oxygen delivery to the myocardium may cause infarction.
Physical findings vary in the patient with AMI. Within the first few hours, the symptoms may be minimal.2 It is therefore important to repeat the nursing assessment at regular intervals to detect and document changes. Chest pain is the most frequently reported discomfort. There are other sources of chest pain (Table 3.2). The onset of chest pain varies in AMI, but it is most often sudden and is described as being in the retrosternal area with radiation to the jaw, neck, or left arm. Characteristically, the descriptor used is "squeezing" or "crushing" pain lasting longer than 15-30 minutes. Some patients describe a feeling of impending death. The chest pain may be associated with nausea; vomiting; indigestion described by the patient as "heartburn"; diaphoresis; syncope; or palpitations. Additionally, some patients present cool, clammy skin and vasoconstriction due to intense catecholamine release. Frequently, an initial hypertension will be followed by normotension or hypotension. Catecholamine reaction may continue for several hours, leading to a decreased urine output as a result of decreased renal perfusion (Table 3.1).
| Table 3.1 Signs and Symptoms of Myocardial Infarction | |
| Chest pain | Sudden onset Retrosternal Radiates Crushing |
| Fear | Feeling of impending death |
| Indigestion | Heartburn Nausea Vomiting |
| Diaphoresis | Cool, clammy skin |
| Catecholamine reaction | Vasoconstriction Hypotension Decreased urine output |
| Syncope | Transient attacks |
Early signs of heart failure may be present with shortness of breath and rales in the chest. As the MI evolves, full-blown failure may occur (page 28). Symptoms vary from the very mild to severe—as in the patient who presents with symptoms of car-diogenic shock.
| Table 3.2 Sources of Chest Pain Other Than Acute Ml Pain | |
| 1. | Cardiac ischemia pain Variant angina (Prinzmetal's) Unstable angina Prolonged myocardial ischemia |
| 2. | Vascular/cardiac pain Aortic aneurysm Pulmonary embolus Pleurisy Acute pericarditis Pneumonia Rupture of great vessel |
| 3. | Noncardiac pain Indigestion Esophageal reflux, esophageal spasm Mediastinal pain Anxiety Disease of stomach, duodenum, gall bladder Hiatal hernia Renal colic, biliary colic Gastric pain Cortosternal syndrome |
Diagnosis of AMI relies on results of laboratory tests, history, and ECG interpretation (Table 3.3). The patient's physical appearance and description of symptoms are the first indicators of AMI. Serial ECGs are recorded to note changes. When possible, an earlier tracing should be obtained for basic data and comparison. Expected changes in ECG following AMI include: (1) a recorded Q wave in the QRS complex (Table 3.4); (2) an ST segment elevation from the baseline; and (3) an inverted T wave.
| Table 3.3 Diagnosis of Acute Myocardial Infarction | ||||
| History | 1. | Description of pain | ||
| 2. | Assessment of signs and symptoms | |||
| ECG changes | 1. | Significant Q waves — ⅓ the size in height of the entire QRS complex | ||
| 2. | Elevation of the ST segment | |||
| 3. | Inversion of the T wave | |||
| Laboratory data | ||||
| 1. | WBC | |||
| 2. | Enzymes | |||
| CPK | Rises in 6 hr | |||
| Normal 2-3 days | ||||
| MB Band—CPK | Elevation | |||
| LDH | Rises in 6-12 hr | |||
| Peaks in 3-6 days | ||||
| SGOT | Rises in 6 hr | |||
| Peaks in 24-36 hr (See Section Six) | ||||
The laboratory data supporting the diagnosis are: (1) white blood cell (WBC) elevation (10-12 K/cm) and (2) an increase in serum enzymes. Three specific enzyme studies are significant. (1) Creatine phospho-kinase (CPK), which begins to rise in about 6 hours and returns to normal within 2-3 days, is by far the best indicator of muscle damage. Normal range is 0-50 units. (2) The isoenzyme MB (MB fraction of CPK), when elevated, is an indicator of myocardial damage. (The skeletal muscle has the MM fraction, and the brain has the BB fraction.) (3) Lactic dehydrogenase (LDH) begins to rise in 6-12 hours, peaks at 2-10 times normal within 3-6 days, and returns to normal in 8-14 days. Normal range is 100-300 units. LDH fractions, LDH1 and LDH2, add specific heart muscle injury data. The normal ratio of LDH1to LDH2is less than 1:1; LDH1is usually lower than LDH2. When the LDH1level rises so that the ratio is greater than 1:1 and the LDH1exceeds the LDH2 (this is termed "flipped") and is combined with a significant rise of the CPK, it is generally considered diagnostic of AMI. LDH1 is relatively cardiospecific, but hepatic disease will also elevate this isoenzyme.
| Table 3.4 Indications of Acute Ml in ECG Tracings by Abnormal Q Waves | |
| Type of AMI | Lead Indicators |
| Diaphragmatic/inferior | π, π τ, AVF |
| Anterolateral | I, AVL, V4, V5, V6 |
| Anterior | pairs — V1-V2, V2-V3, V3-V4, V4-V5, V5-V6 |
| Anteroseptal | V3, V4, V5, AVL |
Serum glutamic-oxaloacetic transaminase (SGOT) begins to rise in 6 hours, peaks at 500-600 units in 24-48 hours, and returns to normal range of 0-50 units within 3-4 days. Enzyme studies contribute to the diagnosis (Section Six).
Complications are common with AMI (Table 3.5). Some are more benign than others.2, 14, 78 In the first category are stable angina, occasional irregular heart beats, and mild congestive failure, all of which are treatable. Of more concern are lethal arrhythmias, ventricular tachycardia, fibrillation, asystole, severe congestive failure, cardiogenic shock, and rupture of papillary muscle or other cardiac tissue. Aggressive pharmacologic intervention, hemodynamic monitoring, the intra-aortic balloon pump, or surgical intervention may be needed to prevent fatal outcomes for these complications.
Therapeutic interventions for AMI include rest, pain control, and administration of oxygen. Morphine sulfate is the drug of choice but is used with caution in patients with an inferior infarction because of vagotonic effect. Vistaril and Phenergan are used in combination with morphine. A reduced amount of narcotic may then be given to control pain, and the gastrointestinal symptoms of nausea and vomiting are controlled. Medications are given intravenously to alleviate interference with enzyme reports that occur with intramuscular injections. Oxygen is administered at 2-4 liters per minute; use of nasal prongs is the preferred method. Patients frequently report a feeling of smothering when a mask is used.
| Table 3.5 Complications Following Acute Myocardial Infarction | |
|
|
Prophylactic lidocaine at a rate of 2-4 mg/min is sometimes ordered as a precautionary intervention. Many protocols rely on bolus administration of 50-100 mg, with two or three given if (1) there are more than six premature ventricular contractions per minute; (2) multiform prematures appear; or (3) the R wave moves in close proximity to the T wave (R on T phenomenon). The bolus injections are then followed with a lidocaine infusion of 3-4 mg minute.
Diet supervision, beginning with liquids and progressing as tolerated with low-fat and low-sodium diets, is another measure of the therapeutic regimen.
In addition to the prevention of progression of the underlying problem, the goals for treatment of CAD are to relieve the discomforting symptoms of the present problem (atherosclerosis, angina, MI), to prevent complications, and to rehabilitate the patient to the quality of life experienced before the acute illness, if this goal is possible.
Nursing ManagementPriorities for nursing care of a patient with an acute myocar-dial infarction are:
Nursing Diagnoses Most Frequently Associated with Acute Myocardial Infarction (Table 3.6)
|
Cardiac failure refers to the inability of the heart to pump enough blood to meet the body's metabolic needs.
| Table 3.6 Nursing Care Plan: The Patient with an Acute Myocardial Infarction | |||
| Nursing Diagnosis | Assessment Data | Expected Outcome | Nursing Interventions |
| Alteration in comfort: pain related to myocardial ischemia | Subjective Data: Patient reports crushing chest pain or anginal equivalent Objective Data: Pain of extended duration Anxious behavior Diaphoresis Facial expression of pain and discomfort |
The patient will verbalize relief from pain. |
|
| Alteration in cardiac output: decreased related to altered conduction | Subjective Data: Patient has chest pain Patient reports dizziness Objective Data: Arrhythmia appears on monitor-PVCs Hypotensive Pale appearance Light headed |
The patient will maintain normal range of cardiac output as evidenced by stable cardiac rate and rhythm. |
|
| Alteration in tissue perfusion: cardiopulmonary related to interruption of arterial flow | Subjective Data: Patient reports feeling of lethargy Patient states hands and feet are cold Reports he is "sweaty" Objective Data: Diaphoresis Falling blood pressure Reduced urine output Diminished peripheral pulses Diminished sensorium |
The patient will maintain normal tissue perfusion as evidenced by improved peripheral circulation. |
|
| Activity intolerance related to reduced cardiac output |
Subjective Data: Patient reports he is tired constantly Objective Data: Facial expression of extreme fatigue Family members are at bedside most of day and evening |
The patient will have uninterrupted rest periods. |
|
| Anxiety related to fear of death | Subjective Data: Patient rings bell frequently Patient states he fears death Objective Data: Facial expression reveals anxiety Patient continues diaphoretic Restless Does not sleep |
The patient will verbalize anxiety with regard to diagnosis, treatment, end effect on life-style; will develop effective coping mechanisms. |
|
| Disturbance in self-concept: self-esteem related to perception of the sick role | Subjective Data: Patient states he will "never be the person he was before" Objective Data: Appearance of dejection Speaks in very low tones Refuses to attempt ADLS |
The patient will be aware that this illness is a temporary situation; will have a restored sense of self-value. |
|
| Alteration in bowel elimination: constipation related to decreased physical activity | Subjective Data: Patient states he has not had a bowel movement since admission Objective Data: Patient attempts bowel movement Strained expression while using bed side commode |
The patient will resume normal bowel movement pattern without strain. |
|
| Knowledge deficit regarding present illness |
Subjective Data: Patient states he is unclear about his heart attack, how it happened, what can be done to prevent heart attack Objective Data: Unable to discuss or describe
|
The patient will verbalize simple anatomy/physiology of the normal heart, signs/symptoms that bear reporting to physician. |
|
A very rapid heart rate (tachycardia) reduces diastolic filling time. Slow heart rates (bradycardia) and rapid ones reduce cardiac output. Coronary artery filling occurs during diastole. Other problems that have been identified are ventricular aneurysm and hypertensive heart disorder. Failure presents in three forms: left ventricular failure, right ventricular failure, and in its most severe form, cardiogenic shock. The onset varies in patients with cardiovascular disease.14
As the heart begins to lose its ability to pump blood at a normal rate, compensatory mechanisms attempt to keep perfusion levels within normal limits. Venous pressure rises, leading to increased ventricular filling and dilatation. Stronger contractions occur due to the greater stretch of the myofibrils. This stretching, over the long period, results in dilatation of the myocardium. The patient may remain in a compensated state for months or years. However, as Staling's Law tells us, a stretched muscle fiber results in a stronger contraction, up to a point. When that point is passed and the contractions are insufficient, another compensation mechanism must be called on. Increased heart rate is another compensatory mechanism. However, diastolic filling, the perfusion period for coronary arteries, is reduced when the heart rate is increased, reducing coronary artery blood flow. Ventricular filling volume is also reduced. Increased heart rate also increases myocardial oxygen demand. This compensatory mechanism may prove more destructive in the failure patient.
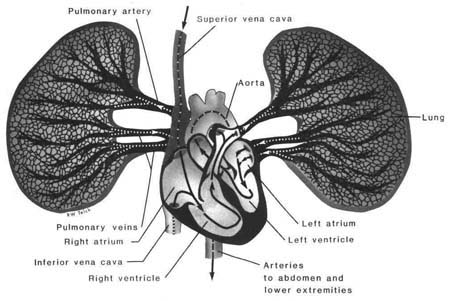
The right and left sides of the heart are independent pumps, so one-sided failure can occur; however, blood travels in a circle, with the right and left heart action occurring in sequence (Fig. 3.2). This anatomic relationship will usually result in eventual transmission of failure from one side to the other. One-sided failure remaining one-sided is rare. It is usually over a very brief period. Generally, left-sided failure precedes right-sided failure. As the left heart fails, output from the left ventricle decreases and blood accumulates within the heart and the pulmonary circulation. Left ventricular and diastolic filling pressure rises and is reflected backward to the pulmonary circulation. The right ventricle is forced to increase pressure for a more forceful contraction. If the pressure remains elevated, the right ventricle will eventually be unable to maintain the increased contraction pressure and will eventually fail. The anatomic relationship accounts for left ventricular failure being the most common cause of right ventricular failure.
The terms forward and backward are sometimes used to describe heart failure. The right ventricle continues to deliver blood to the pulmonary circulation, but the failing left ventricle is unable to eject enough blood into systemic circulation. Pressure builds in the ventricle, back to the atrium, then to the pulmonary vascular bed, and finally to the right heart. This is referred to as backward failure. Pulmonary edema occurs as fluid escapes from the pulmonary vascular bed into the interstitial spaces and the alveoli. Forward failure, or low output failure, refers to inadequate delivery of blood into the arterial system.
|
|
|
Figure 3.2 Right and left heart action |
The etiology of failure is the result of one or more problems within the heart. Although extracardial problems such as anemia and hyperthyroid disease may also be responsible, myocardial infarction with ischemia is the major cause. Additionally, valves that are no longer competent put the patient at risk, as do conduction defects.
Symptoms often depend on the involved ventricle. Typically, the patient reports dyspnea, fatigue, extremity edema, and weight gain. In some patients, the first symptom is a dry cough that progresses to a productive one. Paroxysmal nocturnal dyspnea, (PND) awakening at night unable to breathe, is a common symptom of early failure.
Clinical indicators usually distinguish right and left ventricular failure. Right heart failure is generally associated with failure to accommodate the systemic venous reservoirs, resulting in elevated systemic venous pressure. Nursing assessment reveals jugular venous distention, hepatomegaly, and dependent edema.
Left ventricular failure is associated with an inability to empty the pulmonary venous reservoirs and a reduced stroke volume in the left ventricle. Increased pressure in the pulmonary vascular bed results, as does a reduced cardiac output. The assessment shows a patient with respiratory distress in the form of dyspnea, weakness, dizziness, fatigue, and pulmonary congestion.
The signs and symptoms of right-sided failure (Table 3.7) result from distention of superficial veins (jugular) and the engorgement of body organs, such as the spleen, liver, and kidney. Edema occurs as fluid accumulates in the tissues from the capillaries.
| Table 3.7 Signs and Symptoms of Heart Failure | |
| Left-Sided | Right-Sided |
| Dyspnea | Engorged neck veins |
| Cyanosis | Tachycardia |
| Cough - dry to wet | Edema |
| Tachypnea | Engorged liver |
| Restlessness | Abdominal distention |
| Rales (fine) | Elevated CVP |
| Tachycardia | |
| S3 | |
| Decreased urine output | |
The treatment for cardiac failure includes prompt recognition and treatment of the underlying cause (cardiac or pulmonary). Medication, diet, and fluid regimens are included. Medication regimens for treatment of heart failure vary, but digitalis is recognized as the most important positive inotropic drug in use. It increases contractility of heart muscle and affects the conductivity, automaticity, and refractoriness that give this drug both antiarrhythmic and positive inotropic properties.
Therapeutic intervention in low output heart failure requires medication to increase cardiac output and peripheral perfusion without an increase in oxygen demand. Dopamine at low doses and dobutamine are agents of choice to aid with contractility. Avasodilator agent is added to decrease after load. Nitroprusside or nitroglycerin may be used intravenously in combination with dopamine or dobutamine to accomplish this purpose.
Nursing ManagementPriorities for nursing care of a patient with cardiac failure are:
Nursing Diagnoses Most Frequently Associated with Cardiac Failure
|
The term shock describes a situation in which there is inadequate perfusion of tissues, resulting in hypoxia. When the situation is not rapidly remedied, cellular injury is irreversible. Cardiogenic shock is termed forward failure because there is a severe drop in cardiac output, usually as a result of an acute MI. The ischemic area of the myocardium has reduced contractility, reducing cardiac output.
Cardiogenic shock produces several body responses, the first of which is an attempt to maintain perfusion of the vital organs.57 The release of catecholamines produces a peripheral vascular vasoconstriction. Perfusion of the renal vasculature is also reduced, which, in turn, reduces urine output, an early sign of shock. Cardiogenic shock produces elevated pulmonary capillary wedge pressure and left ventricular and diastolic pressure.
Cardiogenic shock is a complication of acute myocardial infarction due to extensive infarction and necrosis of ventricular myocardium. When 40% or more of the left ventricle is infarcted, the resultant shock state is usually fatal.
Cardiogenic shock may also follow a mechanical defect such as papillary muscle dysfunction with mitral regurgitation, or it may result from ventricular septal rupture of the myocardium.
Various combinations of shock symptoms may be present with Cardiogenic shock. The signs and symptoms associated with Cardiogenic shock are:
|
|
|
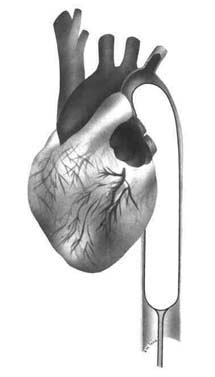
Figure 3.3 Intra-aortic balloon placement |
A pulmonary artery catheter, capable of pressure measurements of the left heart, is useful in regulation of the treatment regimen for Cardiogenic shock.8, 57 The catheter is lodged in a pulmonary artery. Left atrial pressure is measured via a forward occluding balloon (Chapter 4).
Pulmonary artery pressure, wedge pressure, and left ventricular end diastolic pressure can be determined with this catheter. Low arterial pressure and low wedge pressure indicate a need for fluid to expand volume. Saline, plasma, and dextran can be used to correct volume depletion.
The medication regimen frequently includes a sympathomimetic, such as dopamine or dobutamine, in combination with a vasodilator, such as nitroprus-side or nitroglycerin. The rationale for this combination is to administer a drug that decreases preload and after load—the vasodilator—and a drug that increases cardiac contractility. The hypotensive effects of the vasodilator drug are countered with the increase in contractility from the sympathomimetic.
Coronary perfusion and increased cardiac output are the desired effects. A combination of dopamine or dobutamine and nitroprusside is also used when a low arterial pressure with a high wedge pressure occurs. Patients who do not respond to dopamine and nitroprusside require more extensive therapy. An in-tra-aortic balloon pump (Fig. 3.3) insertion may be considered to assist with coronary perfusion and blood pressure support (Table 3.8).
Nursing ManagementPriorities for nursing care of a patient with Cardiogenic shock are:
Nursing Diagnosis Most Frequently Associated with Cardiogenic ShockAlteration in tissue perfusion: cardiopulmonary, renal, peripheral related to left ventricle dysfunction. |
| Table 3.8 Intra-aortic Balloon Pump (IABP) Fig 3.3 |
|
With a normal heart rate of 76 bpm, the ventricles fill, contract, eject blood, and rest to refill within a one-second time period, The coronary arteries receive oxygen and nutrients during the rest period. An IABP is a left ventricular assist device. With precise timing, inflation and deflation of a balloon occurs to enhance cardiac performance. Balloon inflation creates an increase in the arterial pressure during diastole, The increased pressure during diastole increases the blood flow and perfusion to the coronary arteries. Deflation of the balloon creates a decrease in the arterial pressure at the end of diastole, producing a decrease in the workload of the left ventricle. The balloon itself is cylinder-shaped, with one or two chambers mounted on a catheter. The catheter is then threaded upward into the descending thoracic aorta. The approach is usually through the femoral artery. The balloon is positioned with the tip just below the left subclavian artery. Care is taken to place the balloon above the renal arteries in a position to prevent occlusion of these and other arteries. The external end of the catheter is attached to a console that regulates the inflation-deflation cycles of the balloon. It is set to inflate and deflate at the appropriate stages of the cardiac cycle. The balloon setting may be to assist on a 1:1 basis, or it may be set for 1:2,1:3,1:8, whatever is required. The pump is triggered by one of three different signals the ECG, the arterial waveform, or an intrinsic pump rate. The ECG trigger is the most convenient. It uses the R wave as a sensor. The machine is programmed to trigger inflation of the balloon in mid-T wave (diastole) and to deflate just before the QRS complex (systole). For the patient in cardiogenic shock, the deflated balloon during the systolic phase allows the left ventricle to pump blood into the aorta at a lower pressure, The lower pressure is a decrease in resistance—a decreased after load that reduces left ventricular workload. At the same time, blood is pushed back into coronary arteries. In some patients, the IABP has reversed some of the signs and symptoms of cardiogenic shock by increasing peripheral perfusion. The patient suffering a ruptured papillary muscle or ventricular septum may have an enhanced chance for recovery with surgery and the IABP. |
The World Health Organization (WHO) defines an arterial blood pressure of 160/95 mm/Hg or greater on three separate occasions as hypertension and blood pressure between 140/90 and 160/95 mm/Hg as borderline hypertension. Systolic hypertension indicates a systolic pressure greater than 160 mm/Hg and a diastolic pressure of 90 mm/Hg or less. For not clearly understood reasons, the prevalence of hypertension varies with age, gender, race, education, socioeconomic level, and geographic region. For example, in the United States, the prevalence of hypertension increases with age, is greater in blacks than whites, and is more frequently found in males than females until middle age, at which time the ratio reverses. When hypertension is found in blacks, blood pressure levels tend to be higher than those in whites.
Hypertension is an insidious disease, often without symptoms in the early stages. Pressure in the system results partly from the pumping action of the left ventricle. Systolic pressure is the pressure of the left ventricle during contraction. Maximum pressure is reached at this point in the cycle. During the diastolic or resting stage, the pressure in the arterial system falls. Arterial constriction causes an increase in systemic vascular resistance. Pressure rises when cardiac output is elevated and peripheral resistance is high.
Blood pressure above 140 mm/Hg systolic or 90 mm/Hg diastolic in adults is linked to sharp increases in mortality, according to figures assembled by insurance investigators. From records of many subjects in controlled studies, the upper limits of normal for systolic pressures is from 120-149 mm/Hg; for diastolic pressures, it is from 72-88 mm/Hg. Regardless of age, any diastolic pressure above 90 mm/Hg is considered hypertensive. Systolic pressure, a reflection of stroke volume and vessel elasticity, can vary in individuals. Systolic pressure frequently rises with advancing age.
The circulatory system is capable of intrinsic regulation due to the physical properties of its components and autoregulation in each of the tissues it serves.37 It is under the overall integrative control of the autonomic nervous system, which regulates function in response to changing physiologic circumstances. Local factors have important effects on vascular smooth muscle. In metabolically active tissue the release of adenosine, hydrogen, and potassium ion and the consumption of oxygen are assodated with vasodilatation. Adenosine is a very powerful vasodilator and is particularly important in the regulation of coronary blood flow. Vascular smooth muscle cells act in a slow, rhythmic manner, contracting due to spontaneous depolarization. The stretch effect of arterial blood pressure also stimulates contraction of vascular smooth muscles. The sodium ion accumulation in vascular smooth muscle increases the sensitivity to circulating angiotensin II and catecholamines, which in turn add to an elevation of vascular resistance. Another major component in blood pressure regulation is cardiac output. Still others are: (1) blood volume and viscosity; (2) elasticity of the arteries; (3) peripheral resistance; and (4) atherosclerotic disease. The classifications of benign or malignant hypertension are being discarded because these terms do not truly describe the syndrome. Essential or primary hypertension is the terminology used today to describe the large group of patients with pressure elevations for which currently available diagnostic measures cannot pinpoint the underlying pathophysiologic mechanism. Initially, the patient has an increased cardiac output with normal peripheral resistance. As the disease progresses, arteriolar resistance is increased and cardiac output falls to normal or below. Essential hypertension can be further subdivided into classes of severe, moderate, and mild. The division depends on the degree of elevation of diastolic pressure and the extent of involvement of target organs, in particular, the heart, kidneys, brain, and peripheral vasculature. Four factors regulate the hemodynamic pattern in the subgroup:
Secondary hypertension implies that an identifiable pathologic problem is present, resulting in the elevation of blood pressure.37 Classification of secondary hypertension divides this disease entity into vascular, renal parenchymal, neurogenic, and endocrine-metabolic subclasses.
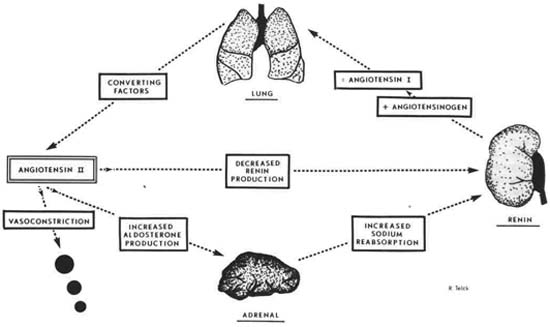
No discussion of hypertension is complete without mention of the renin-angiotensin system. Renin, an enzyme secreted by the juxtaglomerular cells in the kidney in response to a reduced blood flow, initiates the formation of the vasopressor angiotensin I from a plasma protein, angiotensinogen, formed by the liver. During passage through the pulmonary circulation, angiotensin I is lysed by angiotensin converting enzyme (ACE), converting it to angiotensin II, a potent vasopressor (Fig. 3.4). Angiotensin II has several effects, vasoconstriction, facilitation of norepinephrine, and aldosterone release, which in turn causes sodium retention in the distal tubules of the kidney. This renin-angiotensin system helps to maintain blood pressure by increasing effective blood volume, which increases peripheral resistance. Angiotensin II acts directly on the juxtaglomerular cells to inhibit renin release, acting as a control on the system. Any problem that decreases blood pressure, blood volume, or sodium concentration tends to activate this feedback loop system. A hypotensive state, sodium depletion, gastrointestinal fluid or blood loss, or renal artery stenosis all stimulate renin release. Serum renin levels are not elevated in every form of hypertension.
|
|
|
Figure 3.4 Renin-angiotensin system. |
Although the etiology of primary hypertension is thought to be related to atherosclerotic disease, the exact mechanism is unclear. Secondary hypertension is often related to renal parenchymal disease. Renal disorders such as glomerulonephritis, polycystic kidneys, and chronic pyelonephritis account for much of secondary hypertension. Less common, but also potential, causes include pheochromocytoma (adrenal tumor), renal artery stenosis, diabetic nephropathy, and several endocrine disorders. Coarctation of the aorta, a narrowing of the aorta, is also thought to be a cause of secondary hypertension.
| Table 3.9 Nursing Care Plan: The Patient with an Acute Myocardial Infarction | ||||||
| I. | Systolic and diastolic hypertension | |||||
| A. | Primary, essential, or idiopathic | |||||
| B. | Secondary | |||||
| 1. | Renal | |||||
| a. | Renal-parenchymal disease | |||||
| (1) | Acute glomerulonephritis | |||||
| (2) | Chronic nephritis | |||||
| (3) | Polycystic disease | |||||
| (4) | Connective tissue diseases | |||||
| (5) | Diabetic nephropathy | |||||
| (6) | Hydronephrosis | |||||
| 2. | Endocrine | |||||
| a. | Acromegaly | |||||
| b. | Hypothyroidism | |||||
| c. | Hypercalcemia | |||||
| d. | Hyperthyroidism | |||||
| e. | Adrenal | |||||
| (1) | Cortical | |||||
| (a) | Cushing's syndrome | |||||
| (b) | Primary aldosteronism | |||||
| (c) | Congenital adrenal hyperplasia | |||||
| (2) | Medullary: pheochromocytoma | |||||
| f. | Extra-adrenal tumor | |||||
| g. | Carcinoid | |||||
| h. | Exogenous hormones | |||||
| (1) | Estrogen | |||||
| (2) | Glucocorticoids | |||||
| (3) | Mineralocorticoids: licorice | |||||
| (4) | Sympathomimetics | |||||
| (5) | Tyramine-containing foods and MAO inhibitors | |||||
| 3. | Coarctation of the aorta | |||||
| 4. | Pregnancy-induced hypertension | |||||
| 5. | Neurologic disorders | |||||
| a. | Increased intracranial pressure | |||||
| (1) | Brain tumor | |||||
| (2) | Encephalitis | |||||
| (3) | Respiratory acidosis: lung or central nervous system disease | |||||
| b. | Quadriplegia | |||||
| c. | Lead poisoning | |||||
| d. | Guillain-Barre syndrome | |||||
| 6. | Acute stress, including surgery | |||||
| a. | Psychogenic hyperventilation | |||||
| b. | Hypoglycemia | |||||
| c. | Burns | |||||
| d. | Pancreatitis | |||||
| e. | Alcohol withdrawal | |||||
| f. | Sickle cell crisis | |||||
| g. | Postresuscitation | |||||
| h. | Postoperative | |||||
| 7. | Increased intravascular volume | |||||
| 8. | Drugs and other substances | |||||
| II. | Systolic hypertension | |||||
| A. | Increased cardiac output | |||||
| 1. | Aortic valvular regurgitation | |||||
| 2. | Arteriovenous fistula, patent ductus | |||||
| 3. | Thyrotoxicosis | |||||
| 4. | Paget’s disease of bone | |||||
| 5. | Beriberi | |||||
| B. | Rigidity of aorta | |||||
The pathophysiology of the malignant hypertensive state is not clearly understood. The present theory is that conversion to a hypertensive crisis state occurs when increasing levels of blood pressure and an accelerated rate of vascular damage cause a normally negative feedback loop to become a positive loop. An example is the plasma renin cycle.37 Patients with malignant hypertension often have high renin levels that should be low because a rising blood pressure normally is linked to a falling renin level as the body attempts to maintain pressure homeostasis. With high renin levels, angiotensin II and aldosterone levels rise, sodium and water are retained, and effective blood volume increases, all of which should drop renin levels quickly. However, the high pressure probably injures the kidneys, so renin continues to be released in spite of increased blood volume. In this way a negative feedback loop becomes a positive feature in further arterial blood pressure elevation.
There are few signs or symptoms of hypertension. Occasional complaints of headache or lightheadedness may be noted, but unless the patient presents with acute hypertensive crisis and a grossly elevated blood pressure, he or she may be unaware of the presence of the disease. Hypertensive crisis is a life-threatening situation. It should be understood that not all grossly elevated blood pressures are hypertensive crises. An accelerated, or malignant, hypertensive state occurs in about 10% of hypertensive patients. It is a complication of almost all types of primary and secondary hypertension. The presence of severe headache, papilledema, retinopathy with hemorrhages and exudates, renal insufficiency, encephalopathy, and severe elevation of the blood pressure are the diagnostic findings for hypertensive crisis37 (Table 3.10). Hypertensive crisis has a poor prognosis unless treated successfully before vascular damage occurs.
| Table 3.10 Clinical Characteristics of Hypertensive Crisis |
| Blood pressure: Usually greater than 140 mm/Hg diastolic |
| Funduscopic findings: Hemorrhages, exudates, papilledema |
| Neurologic status: Headache, confusion, somnolence, stupor, visual loss, focal deficits, seizures, coma |
| Cardiac findings: Prominent apical impulse, cardiac enlargement, congestive failure |
| Renal: Oliguria, azotemia |
| Gastrointestinal: Nausea, vomiting |
Management of the patient with a hypertensive crisis usually does not require identification of the specific etiology.19The concern is to lower the blood pressure. Hypertensive crisis can be treated with aggressive antihypertensive therapy. The primary aim is the reduction of diastolic blood pressure to a normal range. This is accomplished with attention to maintaining vital organ perfusion.
| Table 3.11 Antihypertensive Agents | |||
|
Type of Drug |
Dosage Range (mg/day) |
||
| Initial | Maximum | ||
| Diuretics | |||
| Thiazides and related sulfonamide diuretics | |||
| Bendroflumethiazide | 2.5 | 5 | |
| Benzthiazide | 25.0 | 50 | |
| Chlorothiazide sodium | 250.0 | 500 | |
| Chlorthalidone | 25.0 | 50 | |
| Cyclothiazide | 1.0 | 2 | |
| Hydrochlorothiazide | 25.0 | 50 | |
| Hydroflumethiazide | 25.0 | 50 | |
| Indapamide | 2.5 | 5 | |
| Methyclothiazide | 2.5 | 5 | |
| Metolazone | 2.5 | 5 | |
| Polythiazide | 2.0 | 4 | |
| Quinethazone | 50.0 | 100 | |
| Trichlormethiazide | 2.0 | 4 | |
| Loop diuretics | |||
| Bumetanide | 0.5 | 10 | |
| Ethacrynic acid | 50.0 | 200 | |
| Furosemide | 80.0 | 480 | |
| Potassium-sparing agents | |||
| Amiloride hydrochloride | 5.0 | 10 | |
| Spironolactone | 50.0 | 100 | |
| Triamterene | 50.0 | 100 | |
| Adrenergic inhibitors | |||
| Beta adrenergic blockers | |||
| Acebutolol | |||
| Atenolol | 25.0 | 100 | |
| Metoprolol tartrate | 50.0 | 300 | |
| Nadolol | 20.0 | 120 | |
| Oxprenolol hydrochloride | 160.0 | 480 | |
| Pindolol | 20.0 | 60 | |
| Propranolol hydrochloride | 40.0 | 480 | |
| Propranolol, long-acting (LA) | 80.0 | 480 | |
| Timolol maleate | 20.0 | 60 | |
| Central-acting adrenergic inhibitors | |||
| Clonidine hydrochloride | 0.2 | 1.2 | |
| Guanabenz acetate | 8.0 | 32 | |
| Methyldopa | 500.0 | 2,000 | |
| Peripheral-acting adrenergic antagonists | |||
| Guanadrel sulfate | 10.0 | 150 | |
| Guanethidine monosulfate | 10.0 | 300 | |
| Rauwolfia alkaloids | |||
| Rauwolfia (whole root) | 50.0 | 100 | |
| Reserpine | 0.05 | 0.25 | |
| Alpha1 adrenergic blocker | |||
| Prazosin hydrochloride | 1.0 | 20 | |
| Combined alpha and beta adrenergic blockers | |||
| Labetalol | 200.0 | 1,200 | |
| Vasodilators | |||
| Hydralazine hydrochloride | 50.0 | 300 | |
| Minoxidil | 5.0 | 100 | |
| Angiotensin-converting enzyme inhibitors | |||
| Captopril | 37.5 | 150 | |
| Enalapril maleate | 10.0 | 40 | |
| Slow-channel calcium-entry blocking agents | |||
| Diltiazem hydrochloride | 120.0 | 240 | |
| Nifedipine | 30.0 | 180 | |
| Verapamil hydrochloride | 240.0 | 480 | |
| Modified from The Joint National Committee on Detection, Elevation, and Treatment of High Blood Pressure. (1984, May). Arch Intern Med, 144.1045-1057. | |||
Care is taken to monitor hemodynamic parameters during the course of treatment. Complications of a too rapid reduction of blood pressure may develop. When significant coronary or cerebrovascular insufficiency is present, angina, cerebral or coronary ischemia, myocardial infarction, or convulsions may follow a precipitous drop in blood pressure. A controlled reduction in the pressure and careful monitoring can avoid these complications.
Parenteral therapy includes the agents with longduration activity, given as a bolus, and the drugs with short duration activity that require constant intravenous infusion to effect a smooth, controlled decrease in the pressure (Table 3.11).
Nursing ManagementTreatment for hypertension includes weight control, dietary restrictions, and long-term medication. Nurses are in ideal settings for identifying people at risk for elevated blood pressure. Blood pressure recording for every patient should be a routine assessment procedure, regardless of the setting. If elevation is present, a referral appointment for proper follow-up should be arranged. Nurses with an appreciation for the prevalence of hypertension in the population, its potential for severe damage to body systems, and the value of control with a long-term medication regimen are in a position to educate patients and families in control and treatment measures for hypertension. Priorities for nursing care of a patient with hypertension are:
Priorities for nursing care of a patient with hypertensive crises are:
Nursing Diagnosis Most Frequently Associated with HypertensionImpaired adjustment related to medical problem requiring life-style alteration. Nursing Diagnosis Most Frequently Associated with Hypertensive CrisisAlteration in tissue perfusion: cerebral, cardiopulmonary, renal, peripheral related to severe vasoconstriction. |
Carditis refers to disease that attacks one of the layers of the heart. There are three types of carditis: endocarditis, pericarditis, and myocarditis.
Infective endocarditis is an infection of the heart's valves and endocardium. It can be subacute, in which a low virulence organism is the etiologic factor, or it may be acute, in which a highly virulent organism is the etiologic factor.
The endothelial layer that covers the heart's chambers and valves is subject to several diseases. Acute bacterial endocarditis usually follows an infection elsewhere. The origin may be bacterial (staphylococcal, pneumococcal, streptococcal, gonococcal, enterococcal), fungal, or rickettsial. Intravenous injections by drug addicts put this population at great risk. The aortic valve is the one most frequently affected by bacteria. Subacute bacterial endocarditis targets patients with established valvular disease, such as rheumatic heart disease, congenitally defective valves, prolapsed valves, or prosthetic valves.9, 25
Acute infective endocarditis is caused by direct invasion of virulent organisms such as staphylococcus or beta-hemolytic streptococcus, leading to deformity of the valve leaflets. The etiology of subcute endocarditis is usually streptococcus viridens.
Acute endocarditis should be suspected when cardiac dysfunction is associated with chills, rapid temperature elevation, and a history of an acute infection.
The onset of subacute endocarditis is similar to the acute form of the disease but varies in severity. Subacute is usually insidious, with intermittent fever, chills, diaphoresis, anorexia, and weight loss. Symptoms develop from the toxic effects of the organism as well as from destruction to the valves with embolization of vegetation fragments. Symptoms of cardiac disease may develop late. Heart murmurs indicative of valve damage are common, along with heart enlargement and congestive failure. Diagnosis is made by blood culture.
Treatment with the appropriate antibiotic, determined by sensitivity studies, may be prolonged and require long-term intravenous therapy. Penicillin is the drug of choice. Fungal infections are treated with amphotericin B. Surgical valve replacement (Chapter 11) is sometimes needed if valve damage is severe.
Pericarditis is an inflammation of the pericardium, the sac covering the heart. It may be chronic or acute and is often a consequence of another pathologic process.
Acute pericarditis is usually accompanied by systemic signs of inflammation. Involvement of nearby myocardial tissues produces changes in the ST segment of an ECG. Chronic pericarditis produces fluid accumulation and compression of the adjacent cardiac structures with impaired cardiac filling. Constrictive pericarditis involves scar tissue development on the epicardium, pericardium, or both. The scar tissue contracts, interfering with cardiac filling. Venous congestion leads to portal hypertension and ascites, without accompanying peripheral edema. Jugular veins are distended.9, 25, 78
Dressier's syndrome, or postmyocardial infarction syndrome, is often referred to as chronic pericarditis. It occurs 1-6 weeks after infarction. It is believed to be due to an immune autoantibody response to pericardial-myocardial antigens exposed to the immune system at the time of the infarction. It is clinically described as fever, pericardial pain, pleuritis, and, occasionally, pneumonitis. Effusion and lung infiltrates may be present. Therapeutic interventions are aspirin, indomethacin, and steroids.
The etiology of pericarditis may be infectious bacteria (streptococcus, gonococcus, meningococcus, staphylococcus), viral (influenza), fungal (myocotic), or parasitic, or it may result from a collagen vascular disease (rheumatic fever, systemic lupus erythematosis). It can also be associated with chest trauma, AMI, metastatic tumors of heart, breast, or lung, or it can be the result of reactions to drugs or immune reactions. The possible etiologies are numerous, but the most prevalent etiology is idiopathic, or nonspecific.
The symptoms of pericarditis are classic. They include a friction rub and pericardial and substernal pain, which is aggravated by movement and breathing. Relief comes when the patient sits up. Fever, chills, and anorexia usually accompany the acute stage. Dyspnea is a frequent symptom. The pericardial friction rub is detected on auscultation but may disappear if fluid fills the pericardial sac. Excess fluid and culture material to determine the etiology are removed via pericardiocentesis. The friction rub is diagnostic. It can be heard as a scratchy sound, synchronous with the heart beat. The diaphragm of the stethoscope is placed in the fourth intercostal space (ICS) at the left sternal border. It is best heard at end expiration.
Chest pain radiating around the scapulae, relieved by bending forward and increasing with movement, is usually indicative. Ah increase in jugular venous pressure and a decrease in the arterial pulse on inspiration, together with a pericardial friction rub, indicate pericarditis with effusion. The third heart sound (S3) suggests progression to constrictive pericarditis.
Treatment is similar to the therapy for endocarditis: relief of pain and administration of an appropriate agent to resolve the inflammatory process. Agents such as aspirin, indomethacin, and ibuprofen are used as nonsteroidal, anti-inflammatory medications. Steroids are also used. Antibiotics are used if the problem is infectious.
Myocarditis is an inflammation of the myocardium. The term suggests involvement of heart muscle by an infective or toxic agent or, possibly, damage by drugs.9, 14, 25
In acute viral heart disease, the damage usually occurs to the myocardium, although the pericardium may also be involved. A necrotic process occurs in the myocardium with destruction of myofibrils and fibrosis. With long-term severe disease, dilatation of the ventricle occurs, but hypertrophy is rare. The pericardium may show some evidence of inflammatory changes without evidence of pericarditis.
Myocarditis is associated with bacterial, viral, fungal, or parasitic invasion. Rheumatic fever is the most common cause. Diagnosis of etiology is difficult if the agent is viral because of the inability to secure tissue from the heart and because the virus tends to disappear from the heart muscle very rapidly. Myocarditis may be linked to systemic diseases such as the collagen-vascular ones, for example, scleroderma or lupus erythematosus.
Symptoms vary with causative agents and degree of damage. These may be so mild as to be overlooked. The patient may be fatigued, dyspneic, tachycardic, febrile, and may have occasional discomfort from palpitations.9 Diagnosis usually follows ventricular enlargement and sudden heart failure. A gallop rhythm, faint heart sounds, systolic murmur, or a friction rub are often detected at this stage. In severe cases, skeletal myalgic pain may occur in conjunction with these symptoms. The cardiovascular symptoms are those of an inappropriate and persistent tachycardia with the gallop rhythm (a summation type). Patients with very severe involvement may develop congestive failure with elevated jugular venous pressure, hepatomegaly, edema, and lung base rales. Differential diagnosis between myocarditis and pericarditis is often difficult. Pericarditis may mask the presence of myocarditis. A systolic murmur suggests mitral or tricuspid regurgitation due to left or right ventricular dilatation with involvement of the myocardium.
Treatment revolves around relieving the myocardial inflammation. Analgesics, anti-inflammatory medications, and antibiotics are given. Treatment of the underlying disease will sometimes bring relief.
Nursing ManagementTreatment involves complete bed rest, comfort measures, administration of an appropriate antibiotic, and digitalis therapy. Prevention of further infection and heart muscle damage is a priority of care. Priorities for nursing care of a patient with carditis are:
Nursing Diagnoses Most Frequently Associated with Carditis
|
Cardiomyopathy refers to myocardial disease that affects the structure and function of the myocardium. It is frequently defined as a disorder of cardiac muscle of unknown cause.
Cardiomyopathies are classified into three main groups on the basis of the structural or functional disorder. The groups are: (1) hypertrophic; (2) dilated (congestive); and (3) restrictive cardiomyopathy.9, 25
Hypertrophic cardiomyopathy is a genetic disorder, characterized by a massive hypertrophy of the left ventricle (occasionally the right) with reduced systolic volume, forceful contractions, increased ventricular stiffness, and impaired relaxation. A common finding is an asymmetrical hypertrophy of the septum. Coronary arteries are usually large, smooth, and patent.
Dilated congestive cardiomyopathy is characterized by severely impaired pumping action of both ventricles with dilatation of the ventricular cavities, with some degree of ventricular hypertrophy. It is a multifactorial syndrome with congestive failure of unknown etiology as the principal aspect.
Restrictive cardiomyopathy is characterized by restriction of ventricular filling, resulting from a very rigid endocardium, subendocardium, or myocardium, the result of a myocardial disease that impairs ventricular distention.
The etiology can be due to a variety of problems (virus, malnutrition, alcoholism). Primary cardiomyopathy refers to involvement of the heart alone. Secondary cardiomyopathy refers to myocardial involvement resulting from other organ system diseases. Examples include thyroid disease, nutritional deficiency, atherosclerotic disease, alcoholism, degenerative myocardial disease, viral infections, and conn-nective tissue disease.14
Hypertrophic cardiomyopathy is a distinct entity. It frequently occurs in the absence of other heart disease or any cause for myocardial hypertrophy. It is thought there may be a connection between catecholamines, endocrine disorder, and hypertrophic cardiomyopathy.
Congestive failure is the most common symptom of cardiomyopathy, along with exertional dyspnea, paroxysmal nocturnal dyspnea (PND), and weakness. Assessment reveals the signs of cardiac failure: edema, hepatic engorgement, gallop rhythm, systemic venous congestion, and tachycardia. Arrhythmias are often present.
Hypertrophic cardiomyopathy has a wide range of symptoms. Some patients are asymptomatic; others show the classic dyspnea on exertion, chest pain resembling angina (at rest or exertional), palpitations, syncope, and dizziness.
Dilated cardiomyopathy has many different symptoms that suggest impaired function in both left and right ventricles. Fatigue on effort occurs, accompanied by dyspnea and linked with other congestive heart failure (CHF) symptoms, such as dependent edema. There is evidence of left ventricular enlargement, as demonstrated by displacement and poor quality sound at the left ventricular apex and a fourth heart sound (S4) resulting from increased left ventricular end diastolic pressure. In the early stage, the diagnosis may depend on detecting cardiac enlargement with gallop rhythm. In the late stage, the clinical picture is one of severe low output cardiac failure with extreme dyspnea; peripheral vasoconstriction as evidenced by cold, cyanotic extremities; small volume arterial pulses; elevated jugular venous pressure; tricuspid regurgitation; and extensive edema in the lower extremities. There may be sacral edema, rales in lung bases, and an enlarged, frequently pulsating liver.
Restrictive cardiomyopathy shows the same CHF symptoms, but this heart failure is of a particular type—it is diastolic impairment. Systolic function remains normal until a late stage. The picture is still of restricted cardiac output with a clinical picture of heart failure. There are commonly third and fourth heart sounds, and mitral regurgitation is common. The systolic murmur tends to recede toward the end of systole if the valve is more competent. When the right ventricle is involved, the appearance suggests constrictive pericarditis. Jugular venous pressure is high. There may be no significant murmur, although tricuspid regurgitation may occur. Advanced cases show ascites, hepatic enlargement, and pleural and pericardial effusion. The ascites is often much greater than lower extremity edema.
Treatment regimens vary. The important issues are: (1) treatment of heart failure; (2) prevention and treatment of arrhythmias; (3) prevention and treatment of embolism; and (4) surgical intervention.
In the acute inflammatory stage of cardiomyopathy, steroids have been ordered. Treatment includes bed rest, with supportive care such as positioning for comfort and ease of breathing; administration of oxygen; restriction of activities and visitors for rest periods; and therapy for the congestive failure. Patients with cardiomyopathy, especially the young and otherwise healthy patient, can be candidates for heart transplant. When atrioventricular valve regurgitation is severe, endocardiectomy and valve replacement have shown improvement.
Nursing ManagementPriorities for nursing care of a patient with cardiomyopathy are:
Nursing Diagnoses Most Frequently Associated with Cardiomyopathy
|
Rheumatic fever is an inflammatory disease of the heart with the ability to involve all of the layers of the heart. Damage to the heart that results from rheumatic fever is called rheumatic heart disease.5 It is generally a delayed complication of an upper respiratory infection.
The immune response to the invasion of streptococcal organisms is thought to be part of the pathogenesis of this disease. The systemic antibody reaction to the invasion may, at a later period, react with cardiac tissue. Some consideration is also given to the collagen effects of the disease. Endocardial involvement is generally limited to the valves. Mitral valve damage is most frequent, with aortic damage in second place. Rarely are the tricuspid or pulmonic valves affected.
Mitral insufficiency, or regurgitation with incompetent valves, allows blood to flow in a retrograde fashion into the left atrium. The workload of the left ventricle increases, causing the compensatory changes of ventricular hypertrophy and dilatation. There is also the additional danger of chordae tendineae involvement and rupture. Mitral stenosis, with fusion or edema of the leaflet junctional areas (the commissures) and shortening of chordae tendineae, restricts the inflow of blood to the ventricle. Left atrial pressure increases and cardiac output is decreased.
Rheumatic fever occurs following an upper respiratory invasion by a (group A) /3-hemolytic streptococcus. It is primarily a disease of children, but any age group is susceptible.
Symptoms vary in this disease. Generally there is a low-grade temperature (100°F) and symptoms of polyarthritis, with swelling, redness, and tenderness in the knees. The episode subsides in 4 weeks. Symptoms of carditis appear in perhaps 3 weeks, with cardiac enlargement, pericardial rub, congestive failure, rapid heart rate, gallop rhythm, and a diastolic murmur. The murmur results from involvement of the mitral valve in the inflammation.
Dyspnea, the most common symptom of mitral stenosis, is associated with an increased pulmonary artery pressure and increased wedge pressure. Pulmonary edema, with resultant right heart failure, may also be present. A mitral stenotic murmur is a rumbling sound heard late in diastole. Mitral insufficiency produces a higher-pitched diastolic murmur. Mitral and aortic murmurs are associated with rheumatic valvular disease.
Edema and inflammation with some scar tissue are frequent sequelae of rheumatic heart disease. Deformity of the valves from fusing and adhering of the leaflets produces hemodynamic alterations. The classic residual of rheumatic fever is a mitral valve lesion. The defect may be either insufficiency with backflow, resulting from inadequate closure of the cusps, or stenosis, resulting in obstructed blood flow due to a narrow, thickened valve opening. Inflammatory processes with scarring or fusing may produce either of these defects.
The treatment regimen for the patient with rheumatic heart disease consists of parenteral antibiotic medication specific to the causative organism, followed by long-term oral administration. Penicillin and erythromycin are the drugs of choice.
Nursing ManagementComfort measures for the signs and symptoms of the acute stage are priorities for nursing intervention. Nursing care includes careful monitoring and frequent assessments for the hospitalized patient. Temperature elevation may precede a recurrent infection or failure to respond to the antibiotic therapy. Blood pressure monitoring will document any sudden change, such as widening pulse pressure. Indicative of progressive aortic regurgitation. Urine output, in addition to recording the amount, is checked for occult hematuria. Assessments are repeated frequently to observe for any side effects of antibiotic agents. Ototoxicity or nephrotoxicity are possible side effects from several medications. As the patient moves from the hospital to the home, patient teaching about the disease and its sequelae is a nursing responsibility. Reinforce the need to continue antibiotic therapy even after the patient feels well. Emphasize longterm treatment and follow-up. Priorities for nursing care of a patient with rheumatic heart disease are:
Nursing Diagnoses Most Frequently Associated with Rheumatic Heart Disease
|
|
|
The pericardiac space normally contains about 10-20 ml of fluid made up of an ultrafiltrate of plasma. It is a part of the extracellular fluid space in the body. An extra amount of pericardial fluid is called pericardial effusion. Cardiac tamponade is a restriction of normal heart activity caused by a compression of the heart due to blood, effusion, or a foreign body in the pericardial space. The return of venous blood to the right heart is restricted, and contraction is impaired. The output of blood from both ventricles may be significantly reduced, leading to a decreased cardiac output.
There are several types of pericardial effusion. Serous effusion is similar to normally occurring fluid. This type occurs with congestive heart failure. It is also found with systemic conditions involving retention of sodium and water and expansion of the extracellular fluid space in the body. An example is those women who develop pericardial effusion during a normal pregnancy.
Serofibrinous effusion is the type most frequently seen when the pericardial effusion is due to the common types of pericarditis (idiopathic, viral, neoplastic). There is a fibrinous deposit on the pericardial surface. The fluid is thin and clear, but there is a high protein concentration.
Bloody pericardial effusion is bleeding into the pericardial space. The principal importance of pericardial effusion is that it may increase the pressure in the pericardial space to create a cardiac tamponade.
Pressure in the pericardial space is normally approximately zero with reference to outside atmospheric pressure. It is similar to intrapleural space pressure. As pericardial fluid accumulates, this pressure rises, slowly at first and then more rapidly as the pericardial limit of distensibility is reached. In traumatic bloody effusion, the pressure rises very quickly. The right-sided heart chambers, the right atrium in particular, have thinner walls and lower inner pressures, and therefore become compressed more rapidly than the chambers of the left heart. Central venous right atrium, right ventricular (diastolic), and pericardial space pressures rise together and are quite equal. When the pressure reaches above 10-12 mm/Hg, pressures in the pulmonary veins, left atrium, and left ventricle (in diastole) also begin to rise, and all intracardiac diastolic pressures are nearly equal. Compression of the heart (tamponade) reduces its size, limits cardiac output, and requires a higher venous pressure to fill the heart. The decrease in arterial pressure that follows is a late secondary effect that represents decompensated tamponade.
A common etiology, diagnosed from the pericardial fluid, is infection with neoplastic disease. Bacterial and tubercular infections and neoplastic pericardial invasions also lead to cardiac tamponade. The most frequent causes include trauma (knife or gunshot wound), perforation of the heart in the course of
AMI or as a complication of a cardiac catheterization procedure, rupture of the aorta into the pericardial space, a coagulation defect, or an anticoagulation therapy defect. Tamponade is usually caused by acute pericarditis but is common in patients with uremic pericardial effusion.
Clinically, the patient will demonstrate an increased venous pressure, a decreased arterial pressure, a narrowing pulse pressure, dyspnea, falling urine output, and a paradoxical pulse pressure of more than 10-15 mm/Hg. Paradoxical pulse is a diagnostic finding of tamponade, as is a widened mediastinal shadow seen on x-ray. With cardiac tamponade, more blood than normal pools in the pulmonary vessels. An exaggerated drop in systolic arterial pressure occurs with inspiration. This response is called paradoxical pulse. Intrathoracic pressure decreases during inspiration of a normal breath, which decreases right atrial pressure and thus allows venous return to the right heart while the pulmonary vasculature expands, producing venous pooling in the lungs. Reduced blood flow moves into the left atrium and left ventricle, producing reduced left ventricular filling, reduced stroke volume, and reduced systolic blood pressure. The normal inspiratory decrease is less than 10 mm/Hg. A paradoxical pulse greater than this is considered abnormal.
The objective is the removal of the fluid. Pericardial fluid may be removed by needle pericardiocentesis or by a surgical technique.
The intervention is based on cause. The choice between needle pericardiocentesis and surgical methods of fluid removal is controversial. Pericardiocentesis is a simple method that can be done at the bedside with local anesthetic, and the patient can be monitored for hemodynamic changes. Care must be taken to prevent further problems with inadvertent puncture of the heart. If surgical drainage of the pericardial fluid is performed, the risk of perforation is minimized, with maximum fluid drainage possible. A larger drain may be placed that will be more effective in draining retained fluid or thick exudate. Subxiphoid pericardiostomy can be performed with local anesthesia. A more extensive procedure for drainage is a left lateral thoracotomy with a partial pericardiectomy. This is called a pericardial window procedure.
Nursing ManagementPriorities for nursing care of a patient with pericardial effusion and cardiac tamponade are:
Nursing Diagnosis Most Frequently Associated with Pericardial Effusion and Cardiac Tamponade |
Alteration In tissue perfusion: cardiopulmonary related to compression of the heart by fluid in the pericardial sac.
Shock is a syndrome in which circulating blood volume is reduced to a level where tissue perfusion is inadequate, resulting in cellular hypoxia. Normal cardiovascular function is dependent on the heart as a pump, blood vessel elasticity, and normal blood volume to maintain homeostatis. Disruption in one of these factors can give rise to shock.
Inadequate tissue perfusion is often a precursor in hypovolemic and cardiogenic shock.8 Cells are dependent for survival on the constant supply of oxygen and nutrition and on the removal of waste products. Shock effects are therefore reflected in cellular metabolism. To understand the mechanism of shock, the work of the elements involved in tissue perfusion should be reviewed.
The closed circuit system of the heart (a pump), the blood, and the vascular and microcirculation system (tubes of distribution) make up the circulatory system. This system is regulated to meet tissue needs. The stages of shock are classified by hemodynamic changes that occur. Early shock is the stage of increased cardiac and sympathetic compensation. Although blood volume may be decreased (hypovolemic) or not available in circulation (neurogenic), this is not sufficient to cause serious problems. The middle stage is characterized as classic shock with its symptoms. Damage to body cells occurs. The late stage is the irreversible shock state when the compensatory measures fail and death is imminent.
Classification of shock is based on clinical consequence, or etiology. Shock may be:
Hypovolemic, caused by blood volume loss;
Cardiogenic, caused by loss of pump action by the heart;
Vasogenic, caused by loss of vascular bed pressure;
Septic, caused by infection.
Regardless of classification, microcirculatory collapse is the common denominator that leads to death when compensatory measures fail. Cellular anoxia is the common link in all shock states. Types of shock are summarized in Table 3.12.
| Table 3.12 Nursing Care Plan: The Patient with an Acute Myocardial Infarction | |||
| Type | Description | Causes | Therapy |
| Cardiogenic | Extensive damage of ventricular myocardium | — Myocardial infarction — Ruptured papillary muscle — Rupture of ventricular tissue |
— Insert PA catheter — Administer fluid, guided by PA values — Administer sympathomimetic drugs — dopamine — dobutamine vasodilators — nitroprusside — NTG — Intra-aortic balloon pump |
| Hypovolemic | Blood volume depletion following blood loss | — Hemorrhage — Excessive diuresis — Severe dehydration — Third spacing |
— Replace fluids — Treat underlying cause |
| Septic | Decreased tissue perfusion and oxygenation allow bacterial invasion | — Death of bacteria-releasing endotoxins — Effects of the bacteria |
— Administer antibiotics — Flush with IV fluids |
| Vasogenic/Neurogenic | Blood volume depletion due to blood pooling in venous beds, microcirculation | — Normal control of BP damaged — Loss of arteriolar tone resulting from continued vasoconstriction |
— Replace fluids |
| Subtype of vasogenic shock | |||
| Anaphylactic | Blood volume depletion due to leakage from intravascular circulation | — Severe antigen-antibody response to release of histamine, serotonin, bradykinin |
— Epinephrine s/c — Bronchodilator — Antihistamine |
| Insulin | Vasodilatation due to altered function in vasomotor center (medulla) | — Lowered blood glucose level |
— Administer a glucose product — orange juice — 50% dextrose |
Hypovolemic shock is a state of blood volume depletion following profound hemorrhage, excessive diuresis, or severe dehydration resulting in loss of whole blood, plasma, and cells. Fluid loss to the third intercostal space, when extracellular fluid is trapped outside the vascular compartment as a result of burns, infection, or intestinal obstruction, may also result in hypovolemic shock.
Compensatory mechanisms are activated as hypovolemic shock deepens. There are three major mechanisms:
In addition to low blood volume when blood is pooled in veins or capillaries, circulating venous return to the heart is reduced. Loss of arteriolar tone with continued venous constriction produces capillary pooling. As the condition progresses, capillary hydrostatic pressure rises, and fluid moves from intravascular to interstitial spaces. Blood volume falls. This type of reduced volume is termed vasogenic shock. It describes a shock state in which there is a loss of vasomotor tone resulting from decreased activity of the vasomotor center in the medulla. There is widespread vasodilatation with increased pooling in vascular beds and decreased systemic pressure. The normal controls of blood pressure are damaged. The term neurogenic refers to the loss of vasomotor tone;vasogenic describes the vasodilatation. Vasogenic shock occurs at the blood vessel level, and neurogenic shock occurs at the vasomotor center.
Vasogenic shock has several forms. Anaphylactic shock, a consequence of severe antigen-antibody response in a highly sensitive patient, is one form. Three substances are released into the blood stream:
(1) histamine, which produces increased capillary permeability and arteriolar dilatation; (2) serotonin, which produces increased capillary permeability and venous constriction; and (3) bradykinin, which causes vasodilatation and increased capillary permeability. These substances affect the blood vessels directly, causing the anaphylaxis. Slow-reacting substances (SRS), also released, cause bronchilar constriction, compounding the problem. Onset is usually only minutes after exposure to the antigen (penicillin, pollen, vaccines, local anesthesia, insect bite). Hypotension and shock symptoms are a consequence of the abrupt onset of vasodilatation and leakage of plasma from intravascular circulation. The course is rapid and must be treated as an emergency, but cellular changes do not occur if the patient receives prompt attention. Epinephrine injection, anti-histamines, and bronchodilators are used for emergency treatment.
Insulin shock is classified as a neurogenic type. Lowered blood glucose levels alter the function of the vasomotor center, resulting in shock symptoms.
Septic shock most frequently occurs as a result of gram-negative bacterial invasion, although a small percentage of patients develop the disease following gram-positive bacteria infection. The major invaders are the aerobic, gram-negative organisms, E. coli, Klebsiella, Enterobacter, Serratia, Proteus, and Pseudo-monas aeruginosa. Shock progresses as the bacteria die, releasing endotoxins. This type of septic shock is called endotoxin shock. The shock state occurs either as a result of the endotoxin release or from the effects of the bacteria. Septic shock can also follow hypovole-mic or cardiogenic shock when decreased tissue perfusion and decreased oxygenation produce failure of the reticuloendothelial system. Invasion of the blood stream by bacteria from the gastrointestinal system occurs because the reticuloendothelial system is unable to detoxify the endotoxins from the gram-negative organisms. A wide spectrum of cardiovascular complications frequently arises when septic shock occurs. Sepsis without hypovolemia, cardiac insufficiency, or lung involvement creates a "warm shock," in which the patient is often warm, and the blood vessels appear to be dilated. There is normal or increased cardiac output with normal or reduced peripheral resistance. Patients are usually hypotensive. Although the mechanism is not clearly understood, the cells involved by the septic process appear to have impaired aerobic and anaerobic metabolism, although there is normal total blood flow with adequate cardiac output. Septic shock in the presence of hypovolemia, cardiac insufficiency, or advanced infectious disease produces a higher peripheral resistance, and these patients may be cold and clammy.
Regardless of the initial event or the type of shock, the symptoms include a combination of:57
The patient in shock may present with all or just a few of the cardinal signs: reduced systolic blood pressure; pale, cool, clammy skin; reduced urine output (below 30 ml/hour); and signs of diminished cerebral perfusion, such as anxiety, confusion, or coma.
Not all shock patients will present with symptoms. At first, various mechanisms of compensation are activated by the body's response system. Falling blood pressure alerts baroreceptors to stimulate the medulla. This in turn causes tachycardia, increased peripheral resistance, and increased circulating blood volume. Blood flow is directed toward maintaining vital organ perfusion. At this stage, cardiac output may be normal due to the increased heart rate. Blood pressure is often very slightly decreased. Orthostatic blood pressure measurements may be used to evaluate whether this is a compensation mechanism working to maintain the blood pressure. If systolic blood pressure varies by 10 mm of mercury or more from a supine to an upright position, the orthostatic drop indicates the body is functioning in a compensated state but is unable to accommodate for a sudden change. Nail beds should also be examined for capillary filling.
Whatever the classification—cardiogenic, hypo-volemic, neurogenic, vasogenic, septic—it indicates only the underlying cause of the shock. In the late stages, all types of shock progress in the same pattern. Tachypnea develops as the condition worsens. Assessment reveals tachycardia with thready pulse, urine output and blood pressure drop, clammy skin, and deterioration of mental status. Hypovolemia is a frequent occurrence in cardiogenic shock following diuretic therapy, as it is in septic shock patients with altered capillary permeability. Without prompt treatment, circulatory volume of the shock patient drops to 60% or lower. The body reacts with very rapid, weak pulse, further drop in blood pressure and urine output, and skin that becomes cold and mottled as circulation is rerouted to vital organs. Cardiogenic shock differs only in filling pressures, which are elevated; the filling pressures in hypovolemic shock and neurogenic shock are normal to low.
With the exception of cardiogenic shock, rapid restoration of intravascular fluid volume is the first priority of therapy. Volume expansion is extremely rapid. Volume expanders are given, including saline (in 3- to 5-liter amounts) and Ringer's lactate solution. The patient is monitored for response to the rapid infusion. A pulmonary artery (PA) catheter is inserted to monitor mean arterial pressure and capillary wedge pressure. For fluid replacement in cardiogenic shock, this is extremely important. Fluid challenges are administered with guidance by the hemodynamic parameters (see Chapter 4). Central venous pressure is also monitored during the rapid fluid administration. Blood plasma expanders are added to the fluid regimen following initial volume deficit replacement. Hypovolemic shock following hemorrhage is treated with whole blood if the hematocrit value falls below 30%. Packed cells are used if myocardial function limits the amount of fluid that can be given.
Sympathomimetic drugs are administered to restore the hemodynamic state. Dopamine, epineph-rine, and norepinephrine, with vasoconstrictor and inotropic properties, are administered for cardiogenic shock. Dopamine is the most frequently used drug to treat shock (see Section Five). Vasodilator therapy is used to relieve severe vasoconstriction in patients who continue with hypotension despite fluid replacement. When profound shock is present, the intra-aortic balloon pump may be used to assist circulation.
Nursing ManagementNursing priorities for care include assessment and evaluation of the patient's response to treatment measures, nursing interventions to aid the medical therapy, and control of the patient's environment. Tissue perfusion may be restored with volume, assistance to the heart, and an assist in altering peripheral resistance with vasodilator or vasoconstricting drugs. Nursing measures are directed at maintenance of adequate respiration by positioning, turning, and monitoring oxygen flow. Fluid infusion, essential to shock treatment, is monitored for flow rate, volume, and patient response. Medication administration may include: (1) antihistamines to treat anaphylactic shock (neurogenic); (2) antibiotics to treat septic shock (neurogenic); or (3) combinations of digitalis, dopamine, and dobutamine for treatment of cardiogenic shock. Medications may be given as additives to the intravenous fluids. Nursing interventions include a well-formed knowledge of the medications—side effects, possible interactions with other drugs, purpose for administration, and expected therapeutic response to the drug. Continuing assessments and evaluation of the patient's response to treatment are important nursing responsibilities for the patient experiencing shock. Priorities for nursing care of a patient with shock are:
Nursing Diagnoses Most Frequently Associated with Shock
|