|
Figure. WHO three-step analgesic ladder
|
| Source: World Health Organization, 1990. Used with permission. |
| Contents | Previous | Next |
One method of classifying pain is by location. Examples of this classification include: somatic pain, visceral pain, referred pain, phantom limb pain and neuralgia.1 Somatic pain is pain that arises from injury or damage to the skin, bone or muscle. It is usually well-localized. In contrast, visceral pain is often caused by pressure or irritation to the internal organs. This pain is poorly localized. Referred pain can be felt in other areas of the body. The pain that radiates to the jaw and down the arm of a person who is having a myocardial infarction is a good example of referred pain. Other types of pain, for which there are poorly understood etiologies, are phantom limb pain, which occurs after an amputation and neuralgia, which follows the path of a nerve.1
It is most helpful to classify pain by duration. Pain can be acute or chronic. Chronic pain is further broken down by etiology. Chronic pain can be malignant or non-malignant. In a review of several textbooks, I discovered that definitions for acute and chronic pain differ. It is important that health care providers adopt a singular definition. For our purpose I have adopted the following definitions.
Acute pain is pain of relatively short duration. It is due to injury or tissue damage and subsides when healing takes place.2 Some examples of acute pain would be seen in patients with an incision, laceration, fracture, bruise or infection.
Acute pain is one of our body's defense mechanisms. It is useful to let the body know that something is wrong. In this sense, acute pain is a symptom of some other pathology. Nursing interventions for acute pain are twofold. First, the nurse is concerned with identification of the cause of the pain and then with the management of the pain. In many cases, treatment of the cause of the acute pain will result in a reduction of the pain. This can easily be seen in a patient with a fracture who experiences some pain relief when the affected limb is immobilized with a splint..
Persons who experience acute pain are often anxious and afraid. The body reacts to acute pain, as it would any other stressor. The heart rate increases, the blood pressure increases, the respiratory rate increases. Blood supply to visceral organs decreases, which may lead to nausea and vomiting. These symptoms reflect the stimulation of the endocrine system as well as the sympathetic nervous system.3 This is the alarm stage of the general adaptation syndrome.
The body could not maintain this heightened state indefinitely, so through adaptation, the body is able to mediate the results of the stressor. The vital signs eventually return to normal and overt symptoms subside. This is the reason that nurses cannot rely on the overt signs seen in the alarm stage for their main source of pain assessment data. It is important to relieve the stressor (pain) as soon as possible, as the body does not have a limitless ability to adapt. If untreated, the body will begin to decompensate, resulting in shock and eventually death.4
Unlike acute pain, chronic pain is a disorder rather than a symptom. Chronic pain persists for six months or longer.5 Chronic pain may be persistent and continuous. It may be decreased with the use of analgesia, but it never truly disappears. A good example of this type of chronic pain is arthritis. Chronic pain may also be intermittent and episodic. Examples of this type of chronic pain include sickle cell crisis, migraine headaches or dysmenorrhea.
Chronic pain is often classified as either malignant or non-malignant. Chronic malignant pain is associated with cancer. Chronic non-malignant pain is also referred to as benign pain. It may have no apparent or diagnosed etiology. The most common example of this type of chronic pain is low back pain. Unlike acute pain, the symptoms associated with chronic pain are more subtle. Chronic pain results in prolonged impairment of mobility, interferes with activities of daily living and decreases quality of life.5 This often results in depression. Persons for whom no pain interventions are effective may become withdrawn or demanding.3
Consider for a moment how you would feel if you were in pain, but since no cause could be found, you were labeled a "quack" or "drug seeker." Patients with chronic pain are often not believed. This is paramount to calling the person a liar. It is not hard to understand why they travel from one health care provider to another looking for help, or why they become hostile, demanding or controlling.
Since chronic pain is so often overlooked, I would like to discuss this area in more detail. In order to understand chronic pain, it is helpful to look at several specific types. In the next section we will look at chronic benign (non-malignant) low back pain, pain related to sickle cell crisis, pain related to arthritis, the pain of headaches and chronic malignant pain associated with cancer.
Characteristics of Acute and Chronic Pain
| Characteristics | Acute Pain | Chronic Pain |
| Length of time and duration | Sudden onset, lasts a predictable length of time | Lasts for longer than 6 months |
| Etiology | Injury resulting in tissue damage | Chronic disease, cancer, or non-defined cause |
| Psychosocial effects | Stress producing, but suffering decreases with time | Depression and feelings of hopelessness |
| Signs and symptoms | Associated with the body's response to stress. May include tachycardia, and hypertension. | Subtle, decreased activity, anorexia, insomnia, anger and decreased quality of life |
| Pattern | Self-limiting | May be continuous or episodic |
| Prognosis | Control is likely | Poor control which leads to increased suffering over time |
| Sources: W. J. Phipps, et al. Medical Surgical Nursing: Concepts and Clinical Practice, 4th ed. (St. Louis: Mosby Year Book, 1991); Smeltzer, S. C. and B. C. Bare, Brunner and Suddarth's Textbook of Medical-Surgical Nursing (Philadelphia: Lippincott, 1992); McCafrery, M. “Pain Assessment and Intervention in Clinical Practice, “ Syllabus, February, 1995. | ||
As an emergency room nurse, I have seen many individuals who present for pain control related to chronic benign low back pain. They express dissatisfaction with the health care system because of its inability to identify a cause and a cure for this condition. Some of these individuals are on disability, are receiving workers' compensation or are in danger of losing their jobs due to excessive absenteeism related to chronic benign low back pain.
It is estimated that 80 percent of the population will experience low back pain at some point in their lives. Many of these will develop chronic benign low back pain, and for some it will affect their activities of daily living and result in permanent disability.6 The effect of chronic benign low back pain on quality of life is tremendous. Chronic low back pain has been associated with depression, alcoholism, drug addiction, impaired functional ability and impaired interpersonal relationships.5
Chronic benign low back pain is one of the leading causes of disability of persons during their working years.6 The economic cost of chronic benign low back pain is seen in the loss of worker productivity, disability and workers' compensation payments. In addition, the cost of medical and health care visits, due to inadequate pain control, place a heavy economic burden on the health care industry.
Persons with chronic benign low back pain are often suspected of trying to "get out of work" or of contributing to their own problem (lack of compliance).5 This attitude by health care workers does nothing to solve the problem. Many factors have been identified as having a relationship to the development of chronic benign low back pain. Height, weight, work habits, types of employment, age and life-style habits have all been suggested to play a part in the development of chronic benign low back pain. In addition, biobehavioral factors such as disease conviction, perceived control, perceived disability, fear of pain, physical stressors, pain tolerance, coping skills and job satisfaction have been related to ability to return to work in patients with chronic benign low back pain.6
As you can see, chronic benign low back pain is a multidimensional phenomena. Treatment varies from one practitioner to another. Treatment may consist of one, or several, of the following modalities: traction, pharmacology, rest, exercise, relaxation, imagery, heat packs, cold packs, biofeedback, acupressure, acupuncture or surgery. Studies related to interventions that increase or decrease the severity of symptoms of chronic benign low back pain are needed to establish the effectiveness of treatment modalities that increase quality of life, satisfaction with health care services and worker productivity.
Causes of Low Back Pain
| Ruptured disk | Pain associated with a ruptured disk is due to the pinching of spinal nerves. Often this problem is the result of injury. The pain classically is described as radiating down the back and into the legs. Numbness and tingling in the lower extremities is also common. |
| Sprains and strains | Pain associated with strains and sprains is often due to injury or poor body mechanics. Heavy lifting may strain the back muscles. In the same way, improper posture will also cause injury to a muscle by increasing the stress placed upon it. |
| Osteoarthritis | Deterioration of the cartilage of the weight-bearing joints can affect the spine. It causes narrowing of the disks. Since osteoarthritis is a frequent finding in the elderly population, it is often mistakenly called a normal sign of aging, m fact, many people demonstrate signs of osteoarthritis on X ray, yet have no related pain. |
| Stress and tension | Back pain has been associated with emotional stress. However, research in this area is limited. |
| Body build | Weight has been suggested to play a part in the development of low back pain. However, for every overweight person I have seen in the emergency room with back pain, I have seen the same number of thin people with low back pain. Also, if low back pain is related to weight, all people with weight problems should be affected with low back pain. Again, much research is needed in this area. |
| Sources: Smeltzer, S. C. and B. C. Bare, Brurmer and Suddarth's Textbook of Medical-Surgical Nursing (Philadelphia: Lippincott, 1992); W. J. Phipps, et al. Medical Surgical Nursing: Concepts and Clinical Practice, 4th ed. (St. Louis: Mosby Year Book, 1991); McCance, K. L., and S. E. Huether, Pathophysiology: The Biological Basis for Disease in Adults and Children. (St. Louis: Mosby Year Book, 1990). | |
Patients who have sickle cell anemia are often under medicated and treated as “drug seekers.” Unlike chronic benign low back pain, the etiology of sickle cell anemia is fairly well understood. The symptoms associated with sickle cell anemia are related to a genetic defect in the hemoglobin molecule. This results in the formation of hemoglobin S instead of the normal hemoglobin A. Physical and emotional stress can cause the cells to sickle due to decreased oxygen tension. Dehydration, infections, cold weather, alcohol and smoking are all linked to episodes of sickle cell pain.7
The problems associated with the abnormal red blood cells are related to tissue hypoxia. Acute manifestations include thrombosis or occlusions in multiple areas of the body. If they occur in the brain, paralysis can result. Pulmonary infarction can be caused by occlusions in the pulmonary vasculature. Occlusion can result in gastrointestinal problems including bowel infarction. The joints in the hands, feet and knees become painful and swollen. Chronic manifestations include retinopathy, blindness, pulmonary hypertension, congestive heart failure, priapism and stasis ulcers of the lower extremities.8
Sickle cell crisis is related to an accelerated rate of sickling. Anything that decreases the amount of oxygen will precipitate this crisis. These deformed cells obstruct the small capillaries; this causes further hypoxia and increases the rate of sickling.9 Tissues hypoxia, due to occlusion, is the major cause of pain in sickle cell crisis. If you have ever used a stair climber, you might have an understanding of the pain that tissue hypoxia can cause. Get on the stair climber and go until your thighs bum so badly that you cannot continue. The pain you are experiencing on the stair climber is due to your muscles getting less oxygen than they need. If you rest, the pain will subside. Now, imagine what it would be like if the pain did not subside. This is the pain associated with sickle cell crisis.
Treatment of this disorder is directed toward prevention of complications and pain control. Remember, pain is a stressor; it causes activation of the sympathetic nervous system. Sympathetic stimulation causes farther hypoxia and increases sickling. It is extremely important to manage pain in these patients.
Patients with sickle cell disease are suspected of being "drug abusers."10 Sickle cell patients often become demanding and controlling. This is probably related to years of trying to obtain adequate pain relief from a reluctant health care system. If your patient is a "clock-watcher," remember that clock-watching is a symptom of poor pain management.11 Consider increasing the dose or frequency of pain medication.
It seems to be common practice in hospitals to treat sickle cell pain with meperidine I.M. Pain related to sickle cell crisis is best treated with morphine. The preferred route is intravenous. When the crisis subsides, the patient may be switched to oral narcotics.12 The intramuscular route causes tissue irritation; eventually over time, the muscle becomes fatty or hard. This interferes with absorption.13 Perhaps, the tolerance that is suspected in patients with sickle cell disease who request increasingly more pain medication, is related more to inadequate absorption than to tolerance.
In addition to pharmacological control of pain, there are several nursing interventions that will help to decrease pain by improving oxygenation. Since dehydration increases the incidence of thrombosis, it is important that the patient's hydration status be monitored closely. Cold temperatures increase sickling, so be sure the patient's room is warm or provide extra blankets. Provide oxygen by nasal canula, and space activities and treatments out, over the day, to prevent fatigue.14 Having, a good understanding of the needs of the patient with sickle cell disease will enable you to provide comfort and prevent complications.
As with other forms of chronic pain, the pain from arthritis causes changes in activities of daily living and perceived quality of life. Depression is not an uncommon finding. People do not adapt to chronic pain. As the pain persists, the perception of pain increases. This leads to insomnia. anorexia, hopelessness and anger.15
Of significance to nurses is the fact that arthritis affects the elderly population in high proportions. When an elderly person becomes confused or non-verbal, such as Alzheimer's patients, nurses often forget to assess and treat their pain. Marzinski, in a recent study of 26 nursing home patients with Alzheimer's, found that only three demonstrated typical pain behaviors. However, patients who were normally moaning became quiet. Patients who were friendly became agitated, and outgoing patients became withdrawn. Her study demonstrates the need to continue to manage pain, even in patients who are unable to verbalize pain.16
There are two major forms of arthritis. Rheumatoid arthritis (inflammatory) and osteoarthritis (degenerative). Both forms of arthritis result in pain and immobility secondary to joint dysfunction.
The cause of rheumatoid arthritis is not known. It has been suggested that it is hereditary. Current theory suggests that it is an autoimmune disorder. Characteristics of rheumatoid arthritis are bilateral joint stiffness (especially in the morning), pain (usually in the hands and feet) and deformity. It can affect people of any age, but is most common between the ages of40-60.17
Treatment goals consist of decreasing inflammation, providing comfort, and maintaining mobility. Current treatment modalities include pharmacology, rest, diet, heat and cold applications and exercise. It is important to note that the best results from anti-inflammatory medications are obtained when a blood level is maintained. Patients need to be instructed to take their medication on a regular basis, rather than p.r.n. Below is a list of arthritis medications and their recommended doses.18
| Aspirin | 1-4.5 g/day |
| Indocin | 75-150 mg/day |
| Clinoril | 300-400 mg/day |
| Tolectin | 1200-1800 mg/day |
| Motrin | 1200-3200 mg/day |
| Nalfon | 2400-3000 mg/day |
| Meclomen | 200-400 mg/day |
| Feldene | 20 mg/day |
| Prednisone | 5-15 mg/day |
| Plaquenil | 200 mg/day |
| Gold (Auranofin) | 6 mg/week |
| Penicillamine | 250-750 mg/day |
| Methotrexate | 5-15 mg/week |
Osteoarthritis is also called degenerative joint disease. Unlike rheumatoid arthritis this is not an inflammatory problem. It usually affects the weight-bearing joints. It is caused by a breakdown in the cartilage. Osteoarthritis occurs to some extent in all people over the age of 60. Unlike rheumatoid arthritis which affects joints bilaterally, Osteoarthritis is asymmetrical. The hip, knee, feet and spine are most often affected. Treatment consists of the administration of non-steroidal anti-inflammatory drugs (NSAIDS) as well as periodic intra-articular cortisone injections. 19
When caring for patients with rheumatoid or Osteoarthritis, it is important for the nurse to provide patient education regarding comfort measures, as well as potential side effects of medications. Salicylates and NSAIDS are hard on the gastric mucosa; patients should be instructed not to take them on an empty stomach. Maintaining adequate blood levels is also important in the control of pain and inflammation, so patients should be told to take the medication around the clock, not just when the pain becomes severe. Patients with a history of gastrointestinal pathology are at risk for bleeding, secondary to gastric ulcers. Instruction on reporting side effects is essential.
Most textbooks that I reviewed state that the use of narcotic analgesia is avoided, due to the possibility of addiction. This may be an unfounded concern. Current research findings do not support this claim.20
Forty-two million people a year seek help for headaches in the United States.21 There are three major types of headaches: migraines (classic or common), cluster headaches and tension headaches. Migraine headaches are more common in women than men. Strong familial tendencies have been demonstrated.22
The classic migraine has three stages: the aura or prodromal phase, the headache itself and the recovery phase. The aura phase is caused by vasoconstriction and is characterized by visual disturbances, light flashes and numbness.23 Migraine headache pain is described as a pulsating or throbbing pain, most often affecting the frontal or temporal areas. Frequency of attacks may be as often as 2-4 a month. They can last for 1-2 days. Associated symptoms include photophobia, sensitivity to noise, nausea and vomiting. Pain associated with migraines is thought to be due to vasodilation of cerebral arteries. Serotonin levels are thought to play a part in this process. Many factors have been suggested as migraine triggers. Bright lights, foods high in tyramine (aged cheese, alcohol and chocolate), and relief of stress may trigger migraines.25 Fatigue, oral contraceptives and menstruation are also triggers.26 The common migraine is similar to the classic migraine, except it lacks a prodromal phase.
Cluster headaches occur more frequently in men than women. They are characterized by severe, localized pain that is constant. They usually start at night and awaken the victim from his sleep. The pain associated with a cluster headache is described as intolerable. The person paces and is unable to sleep or lie down. Some people have considered suicides during episodes of pain.26 Cluster headaches occurs night after night for weeks and months and then disappear for years. Symptoms associated with cluster headaches include watery eyes and nasal congestion. They may last from 15 minutes to 2 hours. Precipitating factors include alcohol ingestion, nitrites, vasodilators and histamines.27
Headache Calendar
Suggested for use with patients who complain of episodic headache pain
|
Date |
__________ | __________ | __________ | __________ | __________ | __________ |
| Did you have a headache today? | yes/no | yes/no | yes/no | yes/no | yes/no | yes/no |
| Did you experience an aura? | yes/no | yes/no | yes/no | yes/no | yes/no | yes/no |
| Blind spots? | yes/no | yes/no | yes/no | yes/no | yes/no | yes/no |
| Flashing lights? | yes/no | yes/no | yes/no | yes/no | yes/no | yes/no |
| Other? (describe below) | yes/no | yes/no | yes/no | yes/no | yes/no | yes/no |
| Rate your pain from 1-10 with 10 being your worst pain | 1 2 3 4 5 6 7 8 9 10 | 1 2 3 4 5 6 7 8 9 10 | 1 2 3 4 5 6 7 8 9 10 | 1 2 3 4 5 6 7 8 9 10 | 1 2 3 4 5 6 7 8 9 10 | 1 2 3 4 5 6 7 8 9 10 |
| What time did your pain begin? Include time (a.m. or p.m.) | ||||||
| What time did your pain end? Include time (a.m. or p.m.) | ||||||
| Duration of pain in hours and minutes | ||||||
| Did you have any of the following symptoms associated with the pain? | ||||||
| Nausea | yes/no | yes/no | yes/no | yes/no | yes/no | yes/no |
| Vomiting | yes/no | yes/no | yes/no | yes/no | yes/no | yes/no |
| Loss of appetite | yes/no | yes/no | yes/no | yes/no | yes/no | yes/no |
| Weakness | yes/no | yes/no | yes/no | yes/no | yes/no | yes/no |
| Dizziness | yes/no | yes/no | yes/no | yes/no | yes/no | yes/no |
| Watery eyes | yes/no | yes/no | yes/no | yes/no | yes/no | yes/no |
| Nasal congestion | yes/no | yes/no | yes/no | yes/no | yes/no | yes/no |
| Light sensitivity | yes/no | yes/no | yes/no | yes/no | yes/no | yes/no |
| Sensitivity to noise | yes/no | yes/no | yes/no | yes/no | yes/no | yes/no |
| Medication taken and times: | ||||||
| Relief after 1 hour (use the pain scale 1-10) | 1 2 3 4 5 6 7 8 9 10 | 1 2 3 4 5 6 7 8 9 10 | 1 2 3 4 5 6 7 8 9 10 | 1 2 3 4 5 6 7 8 9 10 | 1 2 3 4 5 6 7 8 9 10 | 1 2 3 4 5 6 7 8 9 10 |
| What events may have been a trigger for this pain episode? | ||||||
| Foods (chocolate, cheese) | ||||||
| Drinks (alcohol, caffeine) | ||||||
| Emotional stress | ||||||
| Another illness | ||||||
| New medications | ||||||
ADAPTED Source: Foley, K. M. and R.M. Payne. Current Therapy of Pain. (Toronto: B.C. Decker FROM: Inc., 1989)
Tension headaches are due to muscular contraction of neck, scalp and forehead muscles. This condition is associated with vasoconstriction. The pain is described as a tightness that encircles the head. Factors that are associated with tension headaches include stress, fatigue and anxiety. Tension headaches are more common in women.26 This is probably the most common type of headache; it tends to be episodic and chronic. Treatment includes heat, massage, analgesia and muscle relaxants.27
Many people with chronic headaches experience frustration. Patients believe that the headaches are most likely due to a hereditary disorder of the blood vessels; however, physicians tend to contribute the cause to stress. Physicians fail to emphasize headache prevention by identifying triggers. This results in dissatisfaction with the health care system.28
The treatment of vascular headaches such as cluster and migraine headaches, is two-pronged: symptomatic relief and prevention. It might be helpful to discuss several of the medications used for the treatment of headaches in detail.
Ergotamine tartrate is helpful for symptomatic relief if it is given early in the prodromal phase. Ergotamine has a vasocon-strictive action on cerebral vessels. It has little sedative or analgesic action. It can be combined with caffeine to prevent both cluster and migraine headaches. The normal dose is 1-2 mg every 30 minutes until pain subsides or the dose reaches 6 mg. Side effects include nausea, vomiting and thirst. Long-term use may cause intermittent claudication, muscle spasm, weakness and cyanosis of the digits. For this reason it is not recommended for long-term prophylaxsis.29
Imitrex is an ergot alkaloid. It acts as a serotonin receptor agonist. It decreases migraine pain by causing vasoconstriction. It is useful for the treatment of both migraine and cluster headaches. Imitrex also appears to decrease some of the symptoms associated with migraines such as photophobia, nausea and vomiting. The normal dose is 6 mg given subcutaneously. It can be repeated one
time, an hour after the initial dose. It is contraindicated in patients with cardiac disease and hypertension. Side effects include hypertension, chest pain, tingling and drowsiness. It should not be given within 24 hours of an ergot drug. Nurses need to closely monitor a patient during the first dose. Vital signs should be taken every 15 minutes for an hour. The patient also needs to be carefully assessed for chest pain. Pain relief usually begins in about 10 minutes. Imitrex is fairly new, and while it is very effective in some patients, it is not effective for all patients.30
Inderal is a beta blocker. It blocks the effects of the sympathetic nervous system. Its action is not well understood, however, it appears to prevent migraines by preventing cerebral vasodilation. It is contraindicated in patients with heart block, asthma or COPD. Side effects include sleep disturbances, bradycardia, hypotension, dry eyes and dry mouth. The prophylactic dose is 80-240 mg per day in divided doses.31
Methysergide is also an ergot alkaloid. It replaces serotonin on the cranial artery receptor sites, producing vasoconstriction. Side effects of this drug include insomnia, vertigo, peripheral edema, hypotension, flushing and GI upset. Patients should be instructed to report symptoms of abdominal pain, back pain or chest pain. The medication is light-sensitive and should be stored out of the light. The prophylactic dose for the treatment of cluster and migraine headaches is 4-8 mg per day in divided doses. This medication can only be given for 6 months. The patient needs to be off the medication for at least 4 months before resuming treatment.32
In addition to these medications, the acute phase is also treated with analgesia, sedatives and antiemetics. Since the patient is sensitive to light and noise, it is important to place the patient in a quiet, darkened room. Patient teaching and investigation of potential triggers are probably two of the most important components of nursing care for the patient with a history of chronic headaches.
Cancer is not a singular disease. Instead it is a term that is used to describe a group of diseases. Cancer is the result of abnormal cells that multiply at accelerated rates and eventually invade other tissues. Cancer can occur at any place in the body. Individual symptoms vary based on location and stage of the disease. Caring for persons with cancer is a challenge. In addition to the pain caused by the cancer itself, the nurse is faced with managing the pain that results from the various treatment modalities (surgery, radiation and chemotherapy). It is estimated that between 60-96 percent of individuals with cancer experience pain. This pain can be both acute and chronic.33
Cancer pain can be classified as early, intermediate and late stage. Early cancer pain is pain associated with diagnosis and early treatment. It is acute and of short duration. This type of pain is best treated as you would any other pain due to diagnostic tests or surgery. Pain in the intermediate stage is related to treatments such as radiation and chemotherapy. In this stage there may be several different pain sources as a result of therapy. Opportunistic infections, stomatitis and radiation bums are just a few examples. Pain associated with the late stage occurs at the end of the disease. This pain is chronic and slowly increases in intensity. The side effects of chronic pain include fatigue, loss of appetite and decreased mobility. This leads to further inability to tolerate pain.34
Severe chronic pain is most often a late sign and is associated with metastatic cancer. It is identified by patients as the most common symptom that causes the most fear.35 This intractable pain may have several causes, depending upon the area of the body which is affected. Pain may be associated with bone invasion and destruction. This can result in pathological fractures. This pain is described as sharp. The area over the affected bone is sensitive to touch. Pain can also be due to obstruction. Obstruction of the gastrointestinal or urinary system causes a poorly localized, colicky or cramping pain. If the venous, arterial, or the lymph system becomes obstructed it produces a dull aching sensation. Arterial obstruction leads to ischemia, which results in ischmic pain. Compression of nerves causes a sharp, stabbing pain. Infiltration of the cancer to the tissues results in an aching pain.36 Pain may also be due to infection and inflammation, secondary to the cancer or the cancer therapy.37
Table: Common cancer pain syndromes due to peripheral nerve injury
Pain Syndrome |
Associated signs and symptoms |
Affected nerves |
| Tumor infiltration of a peripheral nerve | Constant, burning pain with dysesthesia in an area of sensory loss. Pain is radicular and often unilateral. | Peripheral |
| Postradical neck dissection | Tight, burning sensation in the area of sensory loss. Dysesthesias and shocklike pain may be present. Second type of pain may occur mimicking a drooped shoulder syndrome. |
Cervical plexus |
| Postmastectomy pain | Tight, constricting, burning pain in the posterior arm, axula, and anterior chest wall. Pain exacerbated by arm movement. | Intercostobrachial |
| Post thoracotomy pain | Aching sensation in the distribution of the incision with sensory loss with
or without autonomic changes. Often exquisite point tenderness at the most medial and apical points of the scar with a specific trigger point. Secondary reflex sympathetic dystrophy may develop. |
Intercostal |
| Postnephrectomy pain | Numbness, fullness, or heavyness in the flank, anterior abdomen, and groin. Dysesthesias are common. |
Superficial flank |
| Postlimb amputation | Phantom limb pain usually occurs after pain in the same site before amputation. Stump pain occurs at the site of the surgical scar, several months to years after surgery. It is characterized by a burning dysesthetic sensation that is exacerbated by movement. | Peripheral endings and their central projections |
| Chemotherapy-induced peripheral neuropathy | Painful paresthesias and dysesthesias. Hyporeflexia. Less frequently; motor and sensory loss; rarely: autonomic dysfunction. Commonly associated with the vinca alkaloids, cisplalin, and Taxol. |
Distal areas of peripheral (e.g., polyneuropathy) |
| Radiation-induced peripheral nerve tumors | May promote malignant fibrosarcoma. Painful, enlarging mass in a previously irradiated area. Patients with neurofibromatosis more susceptible. | Superficial and deep |
| Cranial neuropathies | Severe head pain with cranial nerve dysfunction. Leptomeningeal disease. Base of skuff metastasis. |
Cranial V, VII, IX, X, XI, XII are most common |
| Acute and postherpetic neuropathy | Painful paresthesia and dysesthesia. Constant burning and aching pain. Shocklike paroxysmal pain, Immunosuppression from disease or treatment is a risk factor, postherpetic neuropathy incidence increases with age. | Thoracic and cranial (VI) are most common |
Barriers to Cancer Pain Management
| Problems related to health care professionals Inadequate knowledge of pain management Poor assessment of pain Concern about regulation of controlled substances Fear of patient addiction Concern about side effects of analgesics Concern about patients becoming tolerant to analgesics |
| Problems related to patients Reluctance to report pain Concern about distracting physicians from treatment of underlying disease Fear that pain means the disease is worse Concern about not being a "good" patient Reluctance to take pain medication Fear of addiction Worries about side effects Concern about becoming tolerant to pain medication |
| Problems related to the health care system Low priority given to cancer pain treatment Inadequate reimbursement Restrictive regulation of controlled substances Problems of availability of treatment or access to it |
| Source: A. Jacox et al. Management of Cancer Pain: Adults Quick Reference Guide. No. 9. AHCPR Pub. No. 94-0593. Rockville, MD. Agency for Health Care Policy and Research, U.S. Department of Health and Human Services, Public Health Service, March 1994. |
Treatment for cancer pain includes analgesia, surgery to block pain impulses, transcutaneous electrical stimulators (TENS), extravascular narcotic infusion, imagery, relaxation and biofeedback. Individual pain medications and treatment modalities will be discussed later. For our purpose, it is important to discuss the myths associated with the treatment of cancer pain.
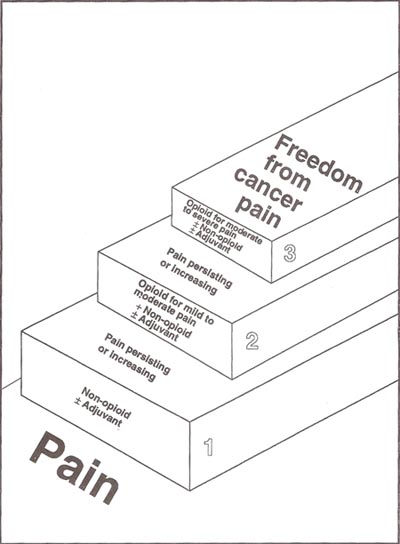
There are two major classifications of cancer analgesics. Narcotic and non-narcotic analgesics. The non-narcotic analgesics are aspirin, acetaminophen, and NSAIDS. NSAIDS cause gas-trointestinal problems, and aspirin cannot be given when the platelet count drops due to the increased incidence of bleeding. The narcotic analgesics are classified by the type of pain they are affective against. Codeine is useful for mild to moderate pain. However, with the severe chronic pain that is seen in the later stages of cancer, codeine is not effective. For severe pain morphine, hydromorphone and methadone are the most effective. The oral route is the preferred route of administration for prolonged narcotic therapy. When managing cancer pain, prevention is the key to success. Cycles such as pain-relief-pain-relief need to be avoided. For this reason, cancer pain is never treated with p.r.n. medication. It is important to maintain a blood level of analgesia to prevent the pain. Contrary to popular belief, tolerance and dependence is not a problem associated with long-term use of narcotics for the treatment of severe chronic cancer pain.38
|
Figure. WHO three-step analgesic ladder
|
| Source: World Health Organization, 1990. Used with permission. |
Morphine does not cause addiction. In addition it is the safest, most effective analgesic for severe pain.39 Sometimes, morphine is not given until very late in the disease because of the mistaken belief that it should be saved to prevent tolerance. This leads to needless suffering by the patient. Nurses are less likely to be concerned with addiction in this patient population than in other populations with chronic pain. However, they are often reluctant to administer adequate amounts of narcotic analgesia due to the belief that it will lead to respiratory depression and death. Morphine, hydromorphone and methadone act at the mu receptor sites, and we know that drugs that act on these sites can cause respiratory depression. In actuality, lethal respiratory depression is not very likely.40 In a study of 401 terminally ill patients receiving high doses of narcotic analgesia, no respiratory depression was found.41 Since more pain medication is required to produce respiratory depression than sedation, nurses should monitor sedation levels. Actually, respiratory depression is more likely to occur following the first dose of a narcotic than after prolonged use.42
Cancer pain, unlike acute pain, is irreversible. As the pain continues, the perception of pain increases. The ability to adapt to pain is decreased with fear and anxiety. The key to managing cancer pain is to provide continuous relief, avoiding peaks and valleys. At the same time it is important to remember to provide sufficient analgesia by administering adequate doses. Needless suffering can be avoided by managing pain for maximum comfort.
Answer the following questions related to specific types of pain.
Answers
1. b
2. a
3. a
4. d
5. d
6. c
7. b
8. d
9. b
10. d
11.d
12. b