|
3. Common Digestive Problems |
v Indigestion
Indigestion, also known as upset stomach or dyspepsia, is discomfort or a burning feeling in the upper abdomen, often accompanied by nausea, abdominal bloating, belching, and sometimes vomiting.
Indigestion might be caused by a disease in the digestive tract, but for many people, it results from eating too much, eating too quickly, eating high-fat foods, or eating during stressful situations. Smoking, drinking too much alcohol, using medications that irritate the stomach lining, being tired, and having ongoing stress can also cause indigestion or make it worse.
Some people have persistent indigestion that is not related to any of these factors. This type of indigestion—called functional or nonulcer dyspepsia—may be caused by a problem in the muscular squeezing action of the stomach (motility).
To diagnose indigestion, the doctor might perform tests for problems, like ulcers. In the process of diagnosis, a person may have x rays of the stomach and small intestine or undergo endoscopy, in which the doctor uses an instrument to look at the inside of the stomach.
Avoiding the foods and situations that seem to cause indigestion in some cases is the most successful way to treat it. Excess stomach acid does not usually cause or result from indigestion, so antacids are not an appropriate treatment, although some people report that they do help. Smokers can help relieve their indigestion by quitting smoking, or at least not smoking right before eating. Exercising with a full stomach may cause indigestion, so scheduling exercise before a meal or at least an hour afterward might help.
To treat indigestion caused by a functional problem in the digestive tract, the doctor may prescribe medicine that affects stomach motility.
Because indigestion can be a sign of or mimic a more serious disease, people should see a doctor if they have
| • | vomiting, weight loss, or appetite loss |
| • | black tarry stools or blood in vomit |
| • | severe pain in the upper right abdomen |
| • | discomfort unrelated to eating |
| • | indigestion accompanied by shortness of breath, sweating, or pain radiating to the jaw, neck, or arm |
v What I Need to Know About Constipation
Disease Definition
Concepts about defecation have been influenced by both social and dietary customs. Hence, the term “constipation” may represent different problems to different individuals. A survey of young adults not seeking health care demonstrated a variety of perceptions about constipation. Of those surveyed, 52 percent believed that constipation meant straining to pass fecal material, and 44 percent believed that constipation was the process of passing hard stools. Other reported perceptions included the inability to defecate when desired (34 percent), infrequent defecation (32 percent) and abdominal discomfort associated with defecation (20 percent). Similarly, a feeling of incomplete evacuation and straining with bowel movements were related to self-reported constipation. In this survey, however, the frequency of defecation was not evaluated.
Defining constipation as hard stools, straining with defecation, or infrequent defecation may be inadequate because some persons with these symptoms may not complain of being constipated. Therefore, constipation can be defined in more general terms as a bothersome difficulty in initiation or completion of defecation. The bother may be due to pain, a decreased frequency or change in bowel function, or the perception that one’s bowel habits are different from normal.
The generally accepted definition of constipation is a frequency of bowel movements of fewer than three per week.
Clinical Presentation and Natural History
Constipation may be caused by a number of different diseases or mechanisms. The known etiologies of constipation include neuropathic disorders, myopathic disorders, mechanical obstruction, metabolic or hormonal disorders, and toxins or drugs. However, these disorders are not observed in most persons in whom constipation has been studied. Hence, the majority of patients suffer from idiopathic constipation. The onset of constipation may occur at any time. It most commonly begins later in life, although the occurrence of constipation in some can be traced to early childhood. Its inception is typically insidious, unrelated to any known initiating event. Early in the course of constipation, infrequent defecation may represent the only symptom. As constipation progresses in severity, however, patients often will develop cramping abdominal pain and bloating that is frequently worse after meals. The pain is usually constant, centered in the lower abdomen, and is not relieved by these patients’ infrequent defecation. Patients who have suffered from constipation for many years may additionally note fatigue, malaise, and decreased appetite. A high fiber diet is typically prescribed for the treatment of this disorder but commonly results only in worsening abdominal pain and bloating.
Because no studies have evaluated the natural history of constipation, its course remains unclear. Unlike other gastrointestinal disorders characterized by intermittent remissions and relapses, constipation appears to be a slowly progressive disorder that rarely resolves. Many severely constipated patients have consumed stimulant laxatives for prolonged periods and often require increasing doses to obtain consistent results. Despite its progressive course, constipation rarely leads to severe morbidity. Hospitalization for constipation is uncommon, and mortality is quite rare. Potential complications of chronic constipation include fecal impaction, fecal incontinence, sigmoid volvulus, and stercoral fecal ulceration. Idiopathic megacolon also may be a complication of chronic constipation. Chronic constipation previously has been thought to be a risk factor for colon cancer. There is, however, no convincing evidence that constipation increases the risk of colon cancer or any other serious illness.
What is constipation?
Constipation means that a person has three bowel movements or fewer in a week. The stool is hard and dry. Sometimes it is painful to pass. You may feel “draggy” and full.
Some people think they should have a bowel movement every day. That is not really true.
There is no “right” number of bowel movements. Each person’s body finds its own normal number of bowel movements. It depends on the food you eat, how much you exercise, and other things.
At one time or another, almost everyone gets constipated. In most cases, it lasts for a short time and is not serious. When you understand what causes constipation, you can take steps to prevent it.
What can I do about constipation?
Changing what you eat and drink and how much you exercise will help relieve and prevent constipation. Here are some steps you can take.
|
|

| 1. | Eat more fiber. Fiber helps form soft, bulky stool. It is found in many vegetables, fruits, and grains. Be sure to add fiber a little at a time, so your body gets used to it slowly. Limit foods that have little or no fiber such as ice cream, cheese, meat, snacks like chips and pizza, and processed foods such as instant mashed potatoes or already-prepared frozen dinners. The chart below lists some high-fiber foods. |
|
|

| High-Fiber Foods | ||
| Fruit | Vegetables | Breads, Cereals, and Beans |
|
apples peaches resberries tangerines |
acorn squash, raw broccoli, raw brussels sprouts, raw cabbage, raw carrots, raw cauliflower, raw spinach, cooked zucchini raw | black-eyed peas, cooked kidney beans, cooked lima beans, cooked whole-grain cereal, cold (all-bran, total, bran flakes) whole-grain cereal, hot (oatmeal, wheatena), whole-wheat or 7-grain bread |
 |
|

| 2. |
Drink plenty of water and other liquids such as fruit and vegetable juices and clear soups. Liquid helps keep the stool soft and easy to pass, so it’s important to drink enough fluids. Try not to drink liquids that contain caffeine or alcohol. Caffeine and alcohol tend to dry out your digestive system. |
 |
| 3. |
Get enough exercise. Regular exercise helps your digestive system stay active and healthy. You don’t need to become a great athlete. A 20- to 30-minute walk every day may help. |
|
| 4. | Allow yourself enough time to have a bowel movement. Sometimes we feel so hurried that we don’t pay attention to our body’s needs. Make sure you don’t ignore the urge to have a bowel movement. | |
| 5. | Use laxatives only if a doctor says you should. Laxatives are medicines that will make you pass a stool. Most people who are mildly constipated do not need laxatives. However, if you are doing all the right things and you are still constipated, your doctor may recommend laxatives for a limited time. Your doctor will tell you if you need a laxative and what type is best for you. Laxatives come in many forms: liquid, chewing gum, pills, and powder that you mix with water, for example. |
|
| 6. | Check with your doctor about any medicines you take. Some medicines can cause constipation. They include calcium pills, pain pills with codeine in them, some antacids, iron pills, diuretics (water pills), and medicines for depression. If you take medicine for another problem, be sure to ask your doctor whether it could cause constipation. | |
Points to Remember
• Constipation affects almost everyone at one time or another.
• Many people think they’re constipated when really they aren’t.
• In most cases, following these simple tips will help prevent constipation:
|
|
Eat a variety of foods, especially beans, bran, whole grains, and fresh fruits and vegetables. |
|
|
Drink plenty of liquids. |
|
|
Exercise regularly. |
|
|
Don’t ignore the urge to have a bowel movement. |
|
|
Understand that normal bowel habits are different for everyone. |
|
|
If your bowel habits change, check with your doctor. |
| • | Most people with mild constipation do not need laxatives. However, doctors may recommend laxatives for a limited time for people with chronic constipation. |
| • | Medicines that you take for another problem might cause constipation. |
v Constipation in Children
As indicated by the percentage of pediatricians involved in diagnosing constipation, children represent a significant fraction of the population suffering from this disorder. Constipation in children, however, seems to be a different entity from that which affects adults. This form of constipation is transient, appears to be slightly more common in boys than girls, demonstrates no specific pathophysiologic correlates, and is thought by pediatricians to be the result of inadequate toilet training and dietary mistakes. Willful suppression of the urge to defecate results in hardening of the stool. Pain on defecation ensues, which leads to further inhibition of defecation. This cycle progresses, often leading to the development of an acute impaction. It is believed that clearing of the impaction, short term treatment with laxatives, and retraining to develop regular bowel habits assist most children in outgrowing this form of constipation..
Constipation means that bowel movements are hard and dry, difficult or painful to pass, and less frequent than usual. It is a common problem for children, but it is usually temporary and no cause for parents to be concerned.
When a child does not eat enough fiber, drink enough liquids, or get enough exercise, constipation is more likely to occur. It also happens when children ignore the urge to have a bowel movement, which they often do out of embarrassment to use a public bathroom, fear or lack of confidence in the absence of a parent, or unwillingness to take a break from play. Sometimes constipation is caused by medicines or a disease.
Symptoms of constipation include
| • | no bowel movement for several days or daily bowel movements that are hard and dry |
| • | cramping abdominal pain |
| • | nausea |
| • | vomiting |
| • | weight loss |
| • | liquid or solid, clay-like stool in the child’s underwear—a sign that stool is backed up in the rectum |
Constipation can make a bowel movement painful, so the child may try to prevent having one. Clenching buttocks, rocking up and down on toes, and turning red in the face are signs of trying to hold in a bowel movement.
Treatment depends on the child’s age and the severity of the problem. Often eating more fiber (fruits, vegetables, whole-grain cereal), drinking more liquids, and getting more exercise will solve the problem. Sometimes a child may need an enema to remove the stool or a laxative to soften it or prevent a future episode. However, laxatives can be dangerous to children and should be given only with a doctor’s approval.
Although constipation is usually harmless, it can be a sign or cause of a more serious problem. A child should see a doctor if
• episodes of constipation last longer than 3 weeks
• the child is unable to participate in normal activities
• small, painful tears appear in the skin around the anus
• a small amount of the intestinal lining is pushed out of the anus (hemorrhoids)
• normal pushing is not enough to expel stool
• liquid or soft stool leaks out of the anus
v Lactose Intolerance
What is lactose intolerance?
Lactose intolerance is the inability to digest significant amounts of lactose, the predominant sugar of milk. This inability results from a shortage of the enzyme lactase, which is normally produced by the cells that line the small intestine. Lactase breaks down milk sugar into simpler forms that can then be absorbed into the bloodstream. When there is not enough lactase to digest the amount of lactose consumed, the results, although not usually dangerous, may be very distressing. While not all persons deficient in lactase have symptoms, those who do are considered to be lactose intolerant.
| Common symptoms include nausea, cramps, bloating, gas, and diarrhea, which begin about 30 minutes to 2 hours after eating or drinking foods containing lactose. The severity of symptoms varies depending on the amount of lactose each individual can tolerate. | 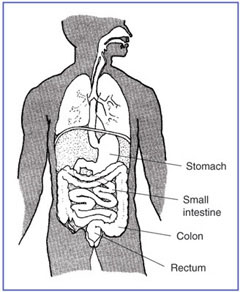 |
| Some causes of lactose intolerance are well known. For instance, certain digestive diseases and injuries to the small intestine can reduce the amount of enzymes produced. In rare cases, children are born without the ability to produce lactase. For most people, though, lactase deficiency is a condition that develops naturally over time. After about the age of 2 years, the body begins to produce less lactase. However, many people may not experience symptoms until they are much older. |
Between 30 and 50 million Americans are lactose intolerant. Certain ethnic and racial populations are more widely affected than others. As many as 75 percent of all African Americans and American Indians and 90 percent of Asian Americans are lactose intolerant. The condition is least common among persons of northern European descent.
Researchers have identified a genetic variation associated with lactose intolerance; this discovery may be useful in developing a diagnostic test to identify people with this condition.
How is lactose intolerance diagnosed?
The most common tests used to measure the absorption of lactose in the digestive system are the lactose tolerance test, the hydrogen breath test, and the stool acidity test. These tests are performed on an outpatient basis at a hospital, clinic, or doctor’s office.
The lactose tolerance test begins with the individual fasting (not eating) before the test and then drinking a liquid that contains lactose. Several blood samples are taken over a 2-hour period to measure the person’s blood glucose (blood sugar) level, which indicates how well the body is able to digest lactose.
Normally, when lactose reaches the digestive system, the lactase enzyme breaks it down into glucose and galactose. The liver then changes the galactose into glucose, which enters the bloodstream and raises the person’s blood glucose level. If lactose is incompletely broken down, the blood glucose level does not rise and a diagnosis of lactose intolerance is confirmed.
The hydrogen breath test measures the amount of hydrogen in a person’s breath. Normally, very little hydrogen is detectable. However, undigested lactose in the colon is fermented by bacteria, and various gases, including hydrogen, are produced. The hydrogen is absorbed from the intestines, carried through the bloodstream to the lungs, and exhaled. In the test, the patient drinks a lactose-loaded beverage, and the breath is analyzed at regular intervals.
Raised levels of hydrogen in the breath indicate improper digestion of lactose. Certain foods, medications, and cigarettes can affect the accuracy of the test and should be avoided before taking it. This test is available for children and adults.
The lactose tolerance and hydrogen breath tests are not given to infants and very young children who are suspected of having lactose intolerance. A large lactose load may be dangerous for the very young because they are more prone to the dehydration that can result from diarrhea caused by the lactose. If a baby or young child is experiencing symptoms of lactose intolerance, many pediatricians simply recommend changing from cow’s milk to soy formula and waiting for symptoms to abate.
If necessary, a stool acidity test, which measures the amount of acid in the stool, may be given to infants and young children. Undigested lactose fermented by bacteria in the colon creates lactic acid and other short-chain fatty acids that can be detected in a stool sample. In addition, glucose may be present in the sample as a result of unabsorbed lactose in the colon.
How is lactose intolerance treated?
Fortunately, lactose intolerance is relatively easy to treat. No treatment can improve the body’s ability to produce lactase, but symptoms can be controlled through diet.
Young children with lactase deficiency should not eat any foods containing lactose. Most older children and adults need not avoid lactose completely, but people differ in the amounts and types of foods they can handle. For example, one person may have symptoms after drinking a small glass of milk, while another can drink one glass but not two. Others may be able to manage ice cream and aged cheeses, such as cheddar and Swiss, but not other dairy products. Dietary control of lactose intolerance depends on people learning through trial and error how much lactose they can handle.
For those who react to very small amounts of lactose or have trouble limiting their intake of foods that contain it, lactase enzymes are available without a prescription to help people digest foods that contain lactose. The tablets are taken with the first bite of dairy food. Lactase enzyme is also available as a liquid. Adding a few drops of the enzyme will convert the lactose in milk or cream, making it more digestible for people with lactose intolerance.
Lactose-reduced milk and other products are available at most supermarkets. The milk contains all of the nutrients found in regular milk and remains fresh for about the same length of time, or longer if it is super-pasteurized.
How is nutrition balanced?
Milk and other dairy products are a major source of nutrients in the American diet. The most important of these nutrients is calcium. Calcium is essential for the growth and repair of bones throughout life. In the middle and later years, a shortage of calcium may lead to thin, fragile bones that break easily, a condition called osteoporosis. A concern, then, for both children and adults with lactose intolerance, is getting enough calcium in a diet that includes little or no milk.
In 1997, the Institute of Medicine released a report recommending new requirements for daily calcium intake. How much calcium a person needs to maintain good health varies by age group. Recommendations from the report are shown in the following table:
| Age group | Amount of calcium to consume daily, in milligrams (mg) |
| 0-6 months | 210 mg |
| 7-12 months | 270 mg |
| 1-3 years | 500 mg |
| 4-8 years | 800 mg |
| 9-18 years | 1,300 mg |
| 19-50 years | 1,000 mg |
| 51-70+ years | 1,200 mg |
Also, pregnant and nursing women under 19 need 1,300 mg daily, while pregnant and nursing women over 19 need 1,000 mg.
In planning meals, making sure that each day’s diet includes enough calcium is important, even if the diet does not contain dairy products. Many nondairy foods are high in calcium. Green vegetables, such as broccoli and kale, and fish with soft, edible bones, such as salmon and sardines, are excellent sources of calcium. To help in planning a high-calcium and low-lactose diet, the table that follows lists some common foods that are good sources of dietary calcium and shows how much lactose they contain.
Recent research shows that yogurt with active cultures may be a good source of calcium for many people with lactose intolerance, even though it is fairly high in lactose. Evidence shows that the bacterial cultures used to make yogurt produce some of the lactase enzyme required for proper digestion.
Clearly, many foods can provide the calcium and other nutrients the body needs, even when intake of milk and dairy products is limited. However, factors other than calcium and lactose content should be kept in mind when planning a diet. Some vegetables that are high in calcium (Swiss chard, spinach, and rhubarb, for instance) are not listed in the chart because the body cannot use the calcium they contain. They also contain substances called oxalates, which stop calcium absorption. Calcium is absorbed and used only when there is enough vitamin D in the body. A balanced diet should provide an adequate supply of vitamin D. Sources of vitamin D include eggs and liver. However, sunlight helps the body naturally absorb or synthesize vitamin D, and with enough exposure to the sun, food sources may not be necessary.
Some people with lactose intolerance may think they are not getting enough calcium and vitamin D in their diet. Consultation with a doctor or dietitian may be helpful in deciding whether any dietary supplements are needed. Taking vitamins or minerals of the wrong kind or in the wrong amounts can be harmful. A dietitian can help in planning meals that will provide the most nutrients with the least chance of causing discomfort.
| Calcium and Lactose in Common Foods | ||
| Foods | Calcium Content | Lactose Content |
| Calcium-fortified orange juice, 1 cup | 308-344 mg | 0 |
| Sardines, with edible bones, 3 oz. | 270 mg | 0 |
| Salmon, canned, with edible bones, 3 oz. | 205 mg | 0 |
| Soymilk, fortified, 1 cup | 200 mg | 0 |
| Broccoli (raw), 1 cup | 90 mg | 0 |
| Orange, 1 medium | 50 mg | 0 |
| Pinto beans, 1/2 cup | 40 mg | 0 |
| Tuna, canned, 3 oz. | 10 mg | 0 |
| Lettuce greens, 1/2 cup | 10 mg | 0 |
| Dairy Products | ||
| Yogurt, plain, low-fat, 1 cup | 415 mg | 5 g |
| Milk, reduced fat, 1 cup | 295 mg | 11 g |
| Swiss cheese, 1 oz. | 270 mg | 1 g |
| Ice cream, 1/2 cup | 85 mg | 6 g |
| Cottage cheese, 1/2 cup | 75 mg | 2-3 g |
| Adapted from Manual of Clinical Dietetics. 6th ed. American Dietetic Association, 2000; and Soy Dairy Alternatives. Available at: www.soyfoods.org. Accessed March 5, 2002. | ||
What is hidden lactose?
Although milk and foods made from milk are the only natural sources, lactose is often added to prepared foods. People with very low tolerance for lactose should know about the many food products that may contain even small amounts of lactose, such as
• bread and other baked goods
• processed breakfast cereals
• instant potatoes, soups, and breakfast drinks
• margarine
• lunch meats (other than kosher)
• salad dressings
• candies and other snacks
• mixes for pancakes, biscuits, and cookies
• powdered meal-replacement supplements
Some products labeled nondairy, such as powdered coffee creamer and whipped toppings, may also include ingredients that are derived from milk and therefore contain lactose.
Smart shoppers learn to read food labels with care, looking not only for milk and lactose among the contents, but also for such words as whey, curds, milk by-products, dry milk solids, and nonfat dry milk powder. If any of these are listed on a label, the product contains lactose.
In addition, lactose is used as the base for more than 20 percent of prescription drugs and about 6 percent of over-the-counter medicines. Many types of birth control pills, for example, contain lactose, as do some tablets for stomach acid and gas. However, these products typically affect only people with severe lactose intolerance.
Summary
Even though lactose intolerance is widespread, it need not pose a serious threat to good health. People who have trouble digesting lactose can learn which dairy products and other foods they can eat without discomfort and which ones they should avoid. Many will be able to enjoy milk, ice cream, and other such products if they take them in small amounts or eat other food at the same time. Others can use lactase liquid or tablets to help digest the lactose. Even older women at risk for osteoporosis and growing children who must avoid milk and foods made with milk can meet most of their special dietary needs by eating greens, fish, and other calcium-rich foods that are free of lactose. A carefully chosen diet, with calcium supplements if the doctor or dietitian recommends them, is the key to reducing symptoms and protecting future health.
|
v Gas in the Digestive Tract |
 |
|
Everyone has gas and eliminates it by burping or passing it through the rectum. However, many people think they have too much gas when they really have normal amounts. Most people produce about 1 to 4 pints a day and pass gas about 14 times a day. Gas is made primarily of odorless vapors—carbon dioxide, oxygen, nitrogen, hydrogen, and sometimes methane. The unpleasant odor of flatulence comes from bacteria in the large intestine that release small amounts of gases that contain sulfur. Although having gas is common, it can be uncomfortable and embarrassing. Understanding causes, ways to reduce symptoms, and treatment will help most people find relief. |
What causes gas?
Gas in the digestive tract (that is, the esophagus, stomach, small intestine, and large intestine) comes from two sources:
| • | swallowed air |
| • | normal breakdown of certain undigested foods by harmless bacteria naturally present in the large intestine (colon) |
Swallowed Air
Air swallowing (aerophagia) is a common cause of gas in the stomach. Everyone swallows small amounts of air when eating and drinking. However, eating or drinking rapidly, chewing gum, smoking, or wearing loose dentures can cause some people to take in more air.
Burping, or belching, is the way most swallowed air—which contains nitrogen, oxygen, and carbon dioxide—leaves the stomach. The remaining gas moves into the small intestine, where it is partially absorbed. A small amount travels into the large intestine for release through the rectum. (The stomach also releases carbon dioxide when stomach acid and bicarbonate mix, but most of this gas is absorbed into the bloodstream and does not enter the large intestine.)
Breakdown of Undigested Foods
The body does not digest and absorb some carbohydrates (the sugar, starches, and fiber found in many foods) in the small intestine because of a shortage or absence of certain enzymes.
This undigested food then passes from the small intestine into the large intestine, where normal, harmless bacteria break down the food, producing hydrogen, carbon dioxide, and, in about one-third of all people, methane. Eventually these gases exit through the rectum.
People who make methane do not necessarily pass more gas or have unique symptoms. A person who produces methane will have stools that consistently float in water. Research has not shown why some people produce methane and others do not.
Foods that produce gas in one person may not cause gas in another. Some common bacteria in the large intestine can destroy the hydrogen that other bacteria produce. The balance of the two types of bacteria may explain why some people have more gas than others.
Which foods cause gas?
Most foods that contain carbohydrates can cause gas. By contrast, fats and proteins cause little gas.
| • | Sugars. The sugars that cause gas are raffinose, lactose, fructose, and sorbitol. |
| • | Raffinose. Beans contain large amounts of this complex sugar. Smaller amounts are found in cabbage, brussels sprouts, broccoli, asparagus, other vegetables, and whole grains. |
| • | Lactose. Lactose is the natural sugar in milk. It is also found in milk products, such as cheese and ice cream, and processed foods, such as bread, cereal, and salad dressing. Many people, particularly those of African, Native American, or Asian background, normally have low levels of the enzyme lactase needed to digest lactose after childhood. Also, as people age, their enzyme levels decrease. As a result, over time people may experience increasing amounts of gas after eating food containing lactose. |
| • | Fructose. Fructose is naturally present in onions, artichokes, pears, and wheat. It is also used as a sweetener in some soft drinks and fruit drinks. |
| • | Sorbitol. Sorbitol is a sugar found naturally in fruits, including apples, pears, peaches, and prunes. It is also used as an artificial sweetener in many dietetic foods and sugarfree candies and gums. |
| • | Starches. Most starches, including potatoes, corn, noodles, and wheat, produce gas as they are broken down in the large intestine. Rice is the only starch that does not cause gas. |
| • | Fiber. Many foods contain soluble and insoluble fiber. Soluble fiber dissolves easily in water and takes on a soft, gel-like texture in the intestines. Found in oat bran, beans, peas, and most fruits, soluble fiber is not broken down until it reaches the large intestine, where digestion causes gas. |
Insoluble fiber, on the other hand, passes essentially unchanged through the intestines and produces little gas. Wheat bran and some vegetables contain this kind of fiber.
What are some symptoms and problems of gas?
The most common symptoms of gas are flatulence, abdominal bloating, abdominal pain, and belching. However, not everyone experiences these symptoms. The determining factors probably are how much gas the body produces, how many fatty acids the body absorbs, and a person’s sensitivity to gas in the large intestine.
Belching
An occasional belch during or after meals is normal and releases gas when the stomach is full of food. However, people who belch frequently may be swallowing too much air and releasing it before the air enters the stomach.
Sometimes a person with chronic belching may have an upper GI disorder, such as peptic ulcer disease, gastroesophageal reflux disease (GERD), or gastroparesis.
Occasionally, some people believe that swallowing air and releasing it will relieve the discomfort of these disorders, and this person may intentionally or unintentionally develop a habit of belching to relieve discomfort.
Gas-bloat syndrome may occur after fundoplication surgery to correct GERD. The surgery creates a one-way valve between the esophagus and stomach that allows food and gas to enter the stomach but often prevents normal belching and the ability to vomit. It occurs in about 10 percent of people who have this surgery but may improve with time.
Flatulence
Another common complaint is passage of too much gas through the rectum (flatulence). However, most people do not realize that passing gas 14 to 23 times a day is normal. Too much gas may be the result of carbohydrate malabsorption.
Abdominal Bloating
Many people believe that too much gas causes abdominal bloating. However, people who complain of bloating from gas often have normal amounts and distribution of gas. They actually may be unusually aware of gas in the digestive tract.
Doctors believe that bloating is usually the result of an intestinal disorder, such as irritable bowel syndrome (IBS). The cause of IBS is unknown, but may involve abnormal movements and contractions of intestinal muscles and increased pain sensitivity in the intestine. These disorders may give a sensation of bloating because of increased sensitivity to gas.
Any disease that causes intestinal inflammation or obstruction, such as Crohn’s disease or colon cancer, may also cause abdominal bloating. In addition, people who have had many operations, adhesions (scar tissue), or internal hernias may experience bloating or pain.
Finally, eating a lot of fatty food can delay stomach emptying and cause bloating and discomfort, but not necessarily too much gas.
Abdominal Pain and Discomfort
Some people have pain when gas is present in the intestine. When pain is on the left side of the colon, it can be confused with heart disease. When the pain is on the right side of the colon, it may mimic gallstones or appendicitis.
What diagnostic tests are used?
Because gas symptoms may be caused by a serious disorder, those causes should be ruled out. The doctor usually begins with a review of dietary habits and symptoms. The doctor may ask the patient to keep a diary of foods and beverages consumed for a specific time period.
If lactase deficiency is the suspected cause of gas, the doctor may suggest avoiding milk products for a period of time. A blood or breath test may be used to diagnose lactose intolerance.
In addition, to determine if someone produces too much gas in the colon or is unusually sensitive to the passage of normal gas volumes, the doctor may ask patients to count the number of times they pass gas during the day and include this information in a diary.
Careful review of diet and the amount of gas passed may help relate specific foods to symptoms and determine the severity of the problem.
Because the symptoms that people may have are so variable, the physician may order other types of diagnostic tests in addition to a physical exam, depending on the patient’s symptoms and other factors.
How is gas treated?
Experience has shown that the most common ways to reduce the discomfort of gas are changing diet, taking medicines, and reducing the amount of air swallowed.
Diet
Doctors may tell people to eat fewer foods that cause gas. However, for some people this may mean cutting out healthy foods, such as fruits and vegetables, whole grains, and milk products.
Doctors may also suggest limiting high-fat foods to reduce bloating and discomfort. This helps the stomach empty faster, allowing gases to move into the small intestine.
Unfortunately, the amount of gas caused by certain foods varies from person to person. Effective dietary changes depend on learning through trial and error how much of the offending foods one can handle.
Nonprescription Medicines
Many nonprescription, over-the-counter medicines are available to help reduce symptoms, including antacids with simethicone. Digestive enzymes, such as lactase supplements, actually help digest carbohydrates and may allow people to eat foods that normally cause gas.
Antacids, such as Mylanta II, Maalox II, and Di-Gel, contain simethicone, a foaming agent that joins gas bubbles in the stomach so that gas is more easily belched away. However, these medicines have no effect on intestinal gas. Dosage varies depending on the form of medication and the patient’s age.
The enzyme lactase, which aids with lactose digestion, is available in caplet and chewable tablet form without a prescription (Lactaid and Lactrase). Chewing lactase tablets just before eating helps digest foods that contain lactose. Also, lactose-reduced milk and other products are available at many grocery stores (Lactaid and Dairy Ease).
Beano, an over-the-counter digestive aid, contains the sugar-digesting enzyme that the body lacks to digest the sugar in beans and many vegetables. The enzyme comes in liquid and tablet form. Five drops are added per serving or 1 tablet is swallowed just before eating to break down the gas-producing sugars. Beano has no effect on gas caused by lactose or fiber.
Prescription Medicines
Doctors may prescribe medicines to help reduce symptoms, especially for people with a disorder such as IBS.
Reducing Swallowed Air
For those who have chronic belching, doctors may suggest ways to reduce the amount of air swallowed. Recommendations are to avoid chewing gum and to avoid eating hard candy. Eating at a slow pace and checking with a dentist to make sure dentures fit properly should also help.
Conclusion
Although gas may be uncomfortable and embarrassing, it is not life-threatening. Understanding causes, ways to reduce symptoms, and treatment will help most people find some relief.
Points to Remember
| • | Everyone has gas in the digestive tract. |
| • | People often believe normal passage of gas to be excessive. |
| • | Gas comes from two main sources: swallowed air and normal breakdown of certain foods by harmless bacteria naturally present in the large intestine. |
| • | Many foods with carbohydrates can cause gas. Fats and proteins cause little gas. |
| • | Foods that may cause gas include |
|
|
beans |
|
|
vegetables, such as broccoli, cabbage, brussels sprouts, onions, artichokes, and asparagus |
|
|
fruits, such as pears, apples, and peaches |
|
|
whole grains, such as whole wheat and bran |
|
|
soft drinks and fruit drinks |
|
|
milk and milk products, such as cheese and ice cream, and packaged foods prepared with lactose, such as bread, cereal, and salad dressing |
|
|
foods containing sorbitol, such as dietetic foods and sugarfree candies and gums |
| • | The most common symptoms of gas are belching, flatulence, bloating, and abdominal pain. However, some of these symptoms are often caused by an intestinal disorder, such as irritable bowel syndrome, rather than too much gas. |
| • | The most common ways to reduce the discomfort of gas are changing diet, taking nonprescription medicines, and reducing the amount of air swallowed. |
| • | Digestive enzymes, such as lactase supplements, actually help digest carbohydrates and may allow people to eat foods that normally cause gas. |
v Bleeding in the Digestive Tract |
 |
|
Bleeding in the digestive tract is a symptom of a disease rather than a disease itself. Bleeding can occur as the result of a number of different conditions, some of which are life threatening. Most causes of bleeding are related to conditions that can be cured or controlled, such as ulcers or hemorrhoids. The cause of bleeding may not be serious, but locating the source of bleeding is important. |
|
|
The digestive or gastrointestinal (GI) tract includes the esophagus, stomach, small intestine, large intestine or colon, rectum, and anus. |
Bleeding can come from one or more of these areas, that is, from a small area such as an ulcer on the lining of the
stomach or from a large surface such as an inflammation of the colon.
Bleeding can sometimes occur without the person noticing it. This type of
bleeding is called occult or hidden. Fortunately, simple tests can detect
occult blood in the stool.
What causes bleeding in the digestive tract?
Stomach acid can cause inflammation that may lead to bleeding at the lower end of the esophagus. This condition, usually associated with the symptom of heartburn, is called esophagitis or inflammation of the esophagus. Sometimes a muscle between the esophagus and stomach fails to close properly and allows the return of food and stomach juices into the esophagus, which can lead to esophagitis. In another, unrelated condition, enlarged veins (varices) at the lower end of the esophagus may rupture and bleed massively. Cirrhosis of the liver is the most common cause of esophageal varices. Esophageal bleeding can be caused by a tear in the lining of the esophagus (Mallory-Weiss syndrome). Mallory-Weiss syndrome usually results from vomiting but may also be caused by increased pressure in the abdomen from coughing, hiatal hernia, or childbirth. Esophageal cancer can cause bleeding.
The stomach is a frequent site of bleeding. Infections with Helicobacter pylori (H. pylori), alcohol, aspirin, aspirin-containing medicines, and various other medicines (NSAIDs) (particularly those used for arthritis) can cause stomach ulcers or inflammation (gastritis). The stomach is often the site of ulcer disease. Acute or chronic ulcers may enlarge and erode through a blood vessel, causing bleeding. Also, patients suffering from burns, shock, head injuries, or cancer, or those who have undergone extensive surgery may develop stress ulcers. Bleeding can also occur from benign tumors or cancer of the stomach, although these disorders usually do not cause massive bleeding.
A common source of bleeding from the upper digestive tract is ulcers in the duodenum (the upper small intestine). Duodenal ulcers are most commonly caused by infection with H. pylori bacteria or drugs such as aspirin or NSAIDs.
In the lower digestive tract, the large intestine and rectum are frequent sites of bleeding.
Hemorrhoids are the most common cause of visible blood in the digestive tract, especially blood that appears bright red. Hemorrhoids are enlarged veins in the anal area that can rupture and produce bright red blood, which can show up in the toilet or on toilet paper. If red blood is seen, however, it is essential to exclude other causes of bleeding since the anal area may also be the site of cuts (fissures), inflammation, or cancer.
Benign growths or polyps of the colon are very common and are thought to be forerunners of cancer. These growths can cause either bright red blood or occult bleeding. Colorectal cancer is the third most frequent of all cancers in the United States and often causes occult bleeding at some time, but not necessarily visible bleeding.
Inflammation from various causes can produce extensive bleeding from the colon. Different intestinal infections can cause inflammation and bloody diarrhea. Ulcerative colitis can produce inflammation and extensive surface bleeding from tiny ulcerations. Crohn’s disease of the large intestine can also produce bleeding.
Diverticular disease caused by diverticula–outpouchings of the colon wall–can result in massive bleeding. Finally, as one gets older, abnormalities may develop in the blood vessels of the large intestine, which may result in recurrent bleeding.
Patients taking blood thinning medications (warfarin) may have bleeding from the GI tract, especially if they take drugs like aspirin.
What are the common causes of bleeding in the digestive tract?
| Esophagus | |
|
|
|
| Stomach | |
|
|
|
| Small Intestine | |
|
|
|
| Large Intestine and Rectum | |
|
|
How is bleeding in the digestive tract recognized?
The signs of bleeding in the digestive tract depend upon the site and severity of bleeding. If blood is coming from the rectum or the lower colon, bright red blood will coat or mix with the stool. The stool may be mixed with darker blood if the bleeding is higher up in the colon or at the far end of the small intestine. When there is bleeding in the esophagus, stomach, or duodenum, the stool is usually black or tarry. Vomited material may be bright red or have a coffee-grounds appearance when one is bleeding from those sites. If bleeding is occult, the patient might not notice any changes in stool color.
If sudden massive bleeding occurs, a person may feel weak, dizzy, faint, short of breath, or have crampy abdominal pain or diarrhea. Shock may occur, with a rapid pulse, drop in blood pressure, and difficulty in producing urine. The patient may become very pale. If bleeding is slow and occurs over a long period of time, a gradual onset of fatigue, lethargy, shortness of breath, and pallor from the anemia will result. Anemia is a condition in which the blood’s iron-rich substance, hemoglobin, is diminished.
How is bleeding in the digestive tract diagnosed?
The site of the bleeding must be located. A complete history and physical examination are essential. Symptoms such as changes in bowel habits, stool color (to black or red) and consistency, and the presence of pain or tenderness may tell the doctor which area of the GI tract is affected. Because the intake of iron, bismuth (Pepto Bismol), or foods such as beets can give the stool the same appearance as bleeding from the digestive tract, a doctor must test the stool for blood before offering a diagnosis. A blood count will indicate whether the patient is anemic and also will give an idea of the extent of the bleeding and how chronic it may be.
Endoscopy
Endoscopy is a common diagnostic technique that allows direct viewing of the bleeding site. Because the endoscope can detect lesions and confirm the presence or absence of bleeding, doctors often choose this method to diagnose patients with acute bleeding. In many cases, the doctor can use the endoscope to treat the cause of bleeding as well.
The endoscope is a flexible instrument that can be inserted through the mouth or rectum. The instrument allows the doctor to see into the esophagus, stomach, duodenum (esophago-duodenoscopy), colon (colonoscopy), and rectum (sigmoidoscopy); to collect small samples of tissue (biopsies); to take photographs; and to stop the bleeding.
Small bowel endoscopy, or enteroscopy, is a procedure using a long endoscope. This endoscope may be used to localize unidentified sources of bleeding in the small intestine.
Other Procedures
Several other methods are available to locate the source of bleeding. Barium x rays, in general, are less accurate than endoscopy in locating bleeding sites. Some drawbacks of barium x rays are that they may interfere with other diagnostic techniques if used for detecting acute bleeding, they expose the patient to x rays, and they do not offer the capabilities of biopsy or treatment.
Angiography is a technique that uses dye to highlight blood vessels. This procedure is most useful in situations when the patient is acutely bleeding such that dye leaks out of the blood vessel and identifies the site of bleeding. In selected situations, angiography allows injection of medicine into arteries that may stop the bleeding.
Radionuclide scanning is a noninvasive screening technique used for locating sites of acute bleeding, especially in the lower GI tract. This technique involves injection of small amounts of radioactive material. Then, a special camera produces pictures of organs, allowing the doctor to detect a bleeding site.
In addition, barium x rays, angiography, and radionuclide scans can be used to locate sources of chronic occult bleeding. These techniques are especially useful when the small intestine is suspected as the site of bleeding since the small intestine may not be seen easily with endoscopy.
How is bleeding in the digestive tract treated?
Endoscopy is the primary diagnostic and therapeutic procedure for most causes of GI bleeding.
Active bleeding from the upper GI tract can often be controlled by injecting chemicals directly into a bleeding site with a needle introduced through the endoscope. A physician can also cauterize, or heat treat, a bleeding site and surrounding tissue with a heater probe or electrocoagulation device passed through the endoscope. Laser therapy is useful in certain specialized situations.
Once bleeding is controlled, medicines are often prescribed to prevent recurrence of bleeding. Medicines are useful primarily for H. pylori, esophagitis, ulcer, infections, and irritable bowel disease. Medical treatment of ulcers, including the elimination of H. pylori, to ensure healing and maintenance therapy to prevent ulcer recurrence can also lessen the chance of recurrent bleeding.
Removal of polyps with an endoscope can control bleeding from colon polyps. Removal of hemorrhoids by banding or various heat or electrical devices is effective in patients who suffer hemorrhoidal bleeding on a recurrent basis. Endoscopic injection or cautery can be used to treat bleeding sites throughout the lower intestinal tract.
Endoscopic techniques do not always control bleeding. Sometimes angiography may be used. However, surgery is often needed to control active, severe, or recurrent bleeding when endoscopy is not successful.
How do you recognize blood in the stool and vomit?
• bright red blood coating the stool
• dark blood mixed with the stool
• black or tarry stool
• bright red blood in vomit
• coffee-grounds appearance of vomit
What are the symptoms of acute bleeding?
• any of bleeding symptoms above
• weakness
• shortness of breath
• dizziness
• crampy abdominal pain
• faintness
• diarrhea
What are the symptoms of chronic bleeding?
• any of bleeding symptoms above
• weakness
• fatigue
• shortness of breath
• lethargy
• faintness
For more information
American College of Gastroenterology (ACG)
4900-B South 31st Street
Alexandria, VA 22206-1656
Phone: 703-820-7400
Fax: 703-931-4520
Email: info@acg.gi.org
Internet: www.acg.gi.org
| v Fecal Incontinence |  |
|
Fecal incontinence is the inability to control your bowels. When you feel the urge to have a bowel movement, you may not be able to hold it until you can get to a toilet. Or stool may leak from the rectum unexpectedly. |
|
|
More than 5.5 million Americans have fecal incontinence. It affects people of all ages—children as well as adults. Fecal incontinence is more common in women than in men and more common in older adults than in younger ones. It is not, however, a normal part of aging. |
|
|
Loss of bowel control can be devastating. People who have fecal incontinence may feel ashamed, embarrassed, or humiliated. Some don’t want to leave the house out of fear they might have an accident in public. Most try to hide the problem as long as possible, so they withdraw from friends and family. |
The social isolation is unfortunate but may be reduced because treatment can improve bowel control and make incontinence easier to manage.
Causes
Fecal incontinence can have several causes:
• constipation
• damage to the anal sphincter muscles
• damage to the nerves of the anal sphincter muscles or the rectum
• loss of storage capacity in the rectum
• diarrhea
• pelvic floor dysfunction
Constipation
Constipation is one of the most common causes of fecal incontinence. Constipation causes large, hard stools to become lodged in the rectum. Watery stool can then leak out around the hardened stool. Constipation also causes the muscles of the rectum to stretch, which weakens the muscles so they can’t hold stool in the rectum long enough for a person to reach a bathroom.
Muscle Damage
Fecal incontinence can be caused by injury to one or both of the ring-like muscles at the end of the rectum called the anal internal and/or external sphincters. The sphincters keep stool inside. When damaged, the muscles aren’t strong enough to do their job, and stool can leak out. In women, the damage often happens when giving birth. The risk of injury is greatest if the doctor uses forceps to help deliver the baby or does an episiotomy, which is a cut in the vaginal area to prevent it from tearing during birth. Hemorrhoid surgery can damage the sphincters as well.
Nerve Damage
Fecal incontinence can also be caused by damage to the nerves that control the anal sphincters or to the nerves that sense stool in the rectum. If the nerves that control the sphincters are injured, the muscle doesn’t work properly and incontinence can occur. If the sensory nerves are damaged, they don’t sense that stool is in the rectum. You then won’t feel the need to use the bathroom until stool has leaked out. Nerve damage can be caused by childbirth, a long-term habit of straining to pass stool, stroke, and diseases that affect the nerves, such as diabetes and multiple sclerosis.
Loss of Storage Capacity
Normally, the rectum stretches to hold stool until you can get to a bathroom. But rectal surgery, radiation treatment, and inflammatory bowel disease can cause scarring that makes the walls of the rectum stiff and less elastic. The rectum then can’t stretch as much and can’t hold stool, and fecal incontinence results. Inflammatory bowel disease also can make rectal walls very irritated and thereby unable to contain stool.
Diarrhea
Diarrhea, or loose stool, is more difficult to control than solid stool that is formed. Even people who don’t have fecal incontinence can have an accident when they have diarrhea.
Pelvic Floor Dysfunction
Abnormalities of the pelvic floor can lead to fecal incontinence. Examples of some abnormalities are decreased perception of rectal sensation, decreased anal canal pressures, decreased squeeze pressure of the anal canal, impaired anal sensation, a dropping down of the rectum (rectal prolapse), protrusion of the rectum through the vagina (rectocele), and/or generalized weakness and sagging of the pelvic floor. Often the cause of pelvic floor dysfunction is childbirth, and incontinence doesn’t show up until the midforties or later.
Diagnosis
The doctor will ask health-related questions and do a physical exam and possibly other medical tests.
| • | Anal manometry checks the tightness of the anal sphincter and its ability to respond to signals, as well as the sensitivity and function of the rectum. |
| • | Anorectal ultrasonography evaluates the structure of the anal sphincters. |
| • | Proctography, also known as defecography, shows how much stool the rectum can hold, how well the rectum holds it, and how well the rectum can evacuate the stool. |
| • | Proctosigmoidoscopy allows doctors to look inside the rectum for signs of disease or other problems that could cause fecal incontinence, such as inflammation, tumors, or scar tissue. |
| • | Anal electromyography tests for nerve damage, which is often associated with obstetric injury. |
Treatment
Treatment depends on the cause and severity of fecal incontinence; it may include dietary changes, medication, bowel training, or surgery. More than one treatment may be necessary for successful control since continence is a complicated chain of events.
Dietary Changes
Food affects the consistency of stool and how quickly it passes through the digestive system. If your stools are hard to control because they are watery, you may find that eating high fiber foods adds bulk and makes stool easier to control. But people with well-formed stools may find that high fiber foods act as a laxative and contribute to the problem. Other foods that may make the problem worse are drinks containing caffeine, like coffee, tea, and chocolate, which relax the internal anal sphincter muscle.
You can adjust what and how you eat to help manage fecal incontinence.
| • | Keep a food diary. List what you eat, how much you eat, and when you have an incontinent episode. After a few days, you may begin to see a pattern involving certain foods and incontinence. After you identify foods that seem to cause problems, cut back on them and see whether incontinence improves. Foods that typically cause diarrhea, and so should probably be avoided, include |
|
|
caffeine |
|
|
cured or smoked meat like sausage, ham, or turkey |
|
|
spicy foods |
|
|
alcohol |
|
|
dairy products like milk, cheese, and ice cream |
|
|
fruits like apples, peaches, or pears |
|
|
fatty and greasy foods |
|
|
sweeteners, like sorbitol, xylitol, mannitol, and fructose, which are found in diet drinks, sugarless gum and candy, chocolate, and fruit juices |
| • | Eat smaller meals more frequently. In some people, large meals cause bowel contractions that lead to diarrhea. You can still eat the same amount of food in a day, but space it out by eating several small meals. |
| • | Eat and drink at different times. Liquid helps move food through the digestive system. So if you want to slow things down, drink something half an hour before or after meals, but not with the meals. |
| • | Eat the right amounts of fiber. For many people, fiber makes stool soft, formed, and easier to control. Fiber is found in fruits, vegetables, and grains, like those listed below. You’ll need to eat 20 to 30 grams of fiber a day, but add it to your diet slowly so your body can adjust. Too much fiber all at once can cause bloating, gas, or even diarrhea. Also, too much insoluble, or undigestible, fiber can contribute to diarrhea. So if you find that eating more fiber makes your diarrhea worse, try cutting back to two servings each of fruits and vegetables and removing skins and seeds from your food. |
| • | Eat foods that make stool bulkier. Foods that contain soluble, or digestible, fiber slow the emptying of the bowels. Examples are bananas, rice, tapioca, bread, potatoes, applesauce, cheese, smooth peanut butter, yogurt, pasta, and oatmeal. |
| • | Get plenty to drink. You need to drink eight 8-ounce glasses of liquid a day to help prevent dehydration and to keep stool soft and formed. Water is a good choice, but avoid drinks with caffeine, alcohol, milk, or carbonation if you find that they trigger diarrhea. |
Over time, diarrhea can rob you of vitamins and minerals. Ask your doctor if you need a vitamin supplement.
|
||||||||
Medication
If diarrhea is causing the incontinence, medication may help. Sometimes doctors recommend using bulk laxatives to help people develop a more regular bowel pattern. Or the doctor may prescribe antidiarrheal medicines such as loperamide or diphenoxylate to slow down the bowel and help control the problem.
Bowel Training
Bowel training helps some people relearn how to control their bowels. In some cases, it involves strengthening muscles; in others, it means training the bowels to empty at a specific time of day.
| • | Use biofeedback. Biofeedback is a way to strengthen and coordinate the muscles and has helped some people. Special computer equipment measures muscle contractions as you do exercises—called Kegel exercises—to strengthen the rectum. These exercises work muscles in the pelvic floor, including those involved in controlling stool. Computer feedback about how the muscles are working shows whether you’re doing the exercises correctly and whether the muscles are getting stronger. Whether biofeedback will work for you depends on the cause of your fecal incontinence, how severe the muscle damage is, and your ability to do the exercises. |
| • | Develop a regular pattern of bowel movements. Some people—particularly those whose fecal incontinence is caused by constipation—achieve bowel control by training themselves to have bowel movements at specific times during the day, such as after every meal. The key to this approach is persistence—it may take a while to develop a regular pattern. Try not to get frustrated or give up if it doesn’t work right away. |
Surgery
Surgery may be an option for people whose fecal incontinence is caused by injury to the pelvic floor, anal canal, or anal sphincter. Various procedures can be done, from simple ones like repairing damaged areas, to complex ones like attaching an artificial anal sphincter or replacing anal muscle with muscle from the leg or forearm. People who have severe fecal incontinence that doesn’t respond to other treatments may decide to have a colostomy, which involves removing a portion of the bowel. The remaining part is then either attached to the anus if it still works properly, or to a hole in the abdomen called a stoma, through which stool leaves the body and is collected in a pouch.
What to do about anal discomfort
The skin around the anus is delicate and sensitive. Constipation and diarrhea or contact between skin and stool can cause pain or itching. Here’s what you can do to relieve discomfort:
| • | Wash the area with water, but not soap, after a bowel movement. Soap can dry out the skin, making discomfort worse. If possible, wash in the shower with lukewarm water or use a sitz bath. Or try a no-rinse skin cleanser. Try not to use toilet paper to clean up—rubbing with dry toilet paper will only irritate the skin more. Premoistened, alcohol-free towelettes are a better choice. |
| • | Let the area air dry after washing. If you don’t have time, gently pat yourself dry with a lint-free cloth. |
| • | Use a moisture barrier cream, which is a protective cream to help prevent skin irritation from direct contact with stool. However, talk to your health care professional before you try anal ointments and creams because some have ingredients that can be irritating. Also, you should clean the area well first to avoid trapping bacteria that could cause further problems. Your health care professional can recommend an appropriate cream or ointment. |
| • | Try using nonmedicated talcum powder or corn starch to relieve anal discomfort. |
| • | Wear cotton underwear and loose clothes that “breathe.” Tight clothes that block air can worsen anal problems. Change soiled underwear as soon as possible. |
| • | If you use pads or disposable undergarments, make sure they have an absorbent wicking layer on top. Products with a wicking layer protect the skin by pulling stool and moisture away from the skin and into the pad. |
Emotional Considerations
Because fecal incontinence can cause distress in the form of embarrassment, fear, and loneliness, taking steps to deal with it is important. Treatment can help improve your life and help you feel better about yourself. If you haven’t been to a doctor yet, make an appointment.
Also, consider contacting the organizations listed at the end of this fact sheet. Such groups can help you find information and support and, in some cases, referrals to doctors who specialize in treating fecal incontinence.
Everyday Practical Tips
Take a backpack or tote bag containing cleanup supplies and a change of clothing with you everywhere.
• Locate public restrooms before you need them so you know where to go.
• Use the toilet before heading out.
• If you think an episode is likely, wear disposable undergarments or sanitary pads.
• If episodes are frequent, use oral fecal deodorants to add to your comfort level.
Fecal Incontinence in Children
If your child has fecal incontinence, you need to see a doctor to determine the cause and treatment. Fecal incontinence can occur in children because of a birth defect or disease, but in most cases it’s because of chronic constipation.
Potty-trained children often get constipated simply because they refuse to go to the bathroom. The problem might stem from embarrassment over using a public toilet or unwillingness to stop playing and go to the bathroom. But if the child continues to hold in stool, the feces will accumulate and harden in the rectum. The child might have a stomachache and not eat much, despite being hungry. And when he or she eventually does pass the stool, it can be painful, which can lead to fear of having a bowel movement.
A child who is constipated may soil his or her underpants. Soiling happens when liquid stool from farther up in the bowel seeps past the hard stool in the rectum and leaks out. Soiling is a sign of fecal incontinence. Try to remember that your child did not do this on purpose. He or she cannot control the liquid stool and may not even know it has passed.
The first step in treating the problem is passing the built-up stool. The doctor may prescribe one or more enemas or a drink that helps clean out the bowel, like magnesium citrate, mineral oil, or polyethylene glycol.
The next step is preventing future constipation. You will play a big role in this part of your child’s treatment. You may need to teach your child bowel habits, which means training your child to have regular bowel movements. Experts recommend that parents of children with poor bowel habits encourage their child to sit on the toilet four times each day (after meals and at bedtime) for 5 minutes. Give rewards for bowel movements and remember that it is important not to punish your child for incontinent episodes.
Some changes in eating habits may be necessary too. Your child should eat more high-fiber foods to soften stool, avoid dairy products if they cause constipation, and drink plenty of fluids every day, including water and juices like prune, grape, or apricot, which help prevent constipation. If necessary, the doctor may prescribe laxatives.
It may take several months to break the pattern of withholding stool and constipation. And episodes may occur again in the future. The key is to pay close attention to your child’s bowel habits. Some warning signs to watch for include
• pain with bowel movements
• hard stool
• constipation
• refusal to go to the bathroom
• soiled underpants
• signs of holding back a bowel movement, like squatting, crossing the legs, or rocking back and forth
Why children get constipated
| • | They were potty-trained too early. |
| • | They refuse to have a bowel movement (because of painful ones in the past, embarrassment, stubbornness, or even a dislike of public bathrooms). |
| • | They are in an unfamiliar place. |
| • | They are reacting to family stress like a new sibling or their parents’ divorce. |
| • | They can’t get to a bathroom when they need to go so they hold it. As the rectum fills with stool, the child may lose the urge to go and become constipated as the stool dries and hardens. |
Hope Through Research
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) conducts and supports research into many kinds of digestive disorders, including fecal incontinence. In addition, researchers throughout the country are working hard to find possible solutions to the problem of fecal incontinence. Some studies address fecal incontinence due to anal sphincter damage and combine surgical procedures with electrical stimulation.
For more information
American Academy of Family Physicians
11400 Tomahawk Creek Parkway
Leawood, KS 66211-2672
Phone: 1-800-274-2237 or (913) 906-6000
Email: fp@aafp.org
Internet: www.aafp.org
American Academy of Pediatrics
National Headquarters
141 Northwest Point Boulevard
Elk Grove Village, IL 60007-1098
Phone: (847) 434-4000
Fax: (847) 434-8000
Internet: www.aap.org
American Dietetic Association (ADA)
120 South Riverside Plaza, Suite 2000
Chicago, IL 60606-6995
Phone: 1-800-366-1655 or 1-800-877-1600
Fax: (312) 899-4899
Internet: www.eatright.org
American Gastroenterological Association
National Office
4930 Del Ray Avenue
Bethesda, MD 20814
Phone: (301) 654-2055
Fax: (301) 652-3890
Email: webinfo@gastro.org
Internet: www.gastro.org
International Foundation for Functional Gastrointestinal Disorders Inc.
P.O. Box 170864
Milwaukee, WI 53217
Phone: 1-888-964-2001 or (414) 964-1799
Fax: (414) 964-7176
Email: iffgd@iffgd.org
Internet: www.iffgd.org
v Infectious Diarrheas
Summary
Infectious diarrheas are the leading cause of morbidity and mortality worldwide and the second most common class of illnesses in the United States after respiratory infections. An estimated 99 million episodes occur annually in the United States, resulting in 8 to 12 million physician consultations; 462,000 to 728,000 hospitalizations; 5 to 8 million prescriptions; 25 to 43 million restricted-activity days, including 7.3 million lost workdays, 4.8 million lost school-days, and 5.8 million bed-days; and 3,100 deaths. Infectious diarrheas are associated with 9 percent of hospitalizations for children under 5 years of age and 1.5 percent of hospitalizations of adults age 20 years and older. Recent survey data suggest the incidence rate of infectious diarrhea is increasing.
Unlike most other digestive diseases, infectious diarrheas are communicable and can spread endemically or in epidemics through households, schools, and communities via person-to-person spread or contaminated food and water. Children less than 5 years of age and those ages 20-39 years are at highest risk of developing illness, while children less than 5 years of age and older adults are at highest risk for hospitalization and death. Infectious diarrheas are a particular problem among child day-care centers; institutional settings (hospitals, long-term care); international travelers; immunocompromised persons, including those with acquired immunodeficiency syndrome (AIDS); and parents and caretakers of children.
General prevention measures include hand washing, good personal hygiene, better animal production and slaughter practices, proper food handling practices, and properly treated water. Treatment to prevent dehydration is similar regardless of the specific cause and includes replacement of fluids and electrolytes and refeeding in children. Antimicrobials are recommended for a few selected infections, but drugs that affect bowel motility rarely are indicated.
Definition and Diagnosis
Infectious diarrhea is a syndrome defined as an increase in the frequency, fluidity, or volume of bowel movements relative to the usual habit that is presumed to be infectious in cause. “Infectious gastroenteritis” describes a clinical presentation of diarrhea or vomiting; these symptoms frequently occur together. “Enteric (or intestinal) infections” most frequently result in diarrhea or gastroenteritis but less frequently can cause systemic symptoms without either.
Infectious diarrhea can be very mild and inconsequential or severe and debilitating and can last from a few days (acute) to several weeks or months (chronic). It often is accompanied by other complaints such as anorexia, malaise, nausea, vomiting, abdominal pain, headache, myalgia, or fever.
There are three categories of agents that cause infectious diarrhea: viral, bacterial, and protozoal. These agents can cause diarrhea by three general mechanisms.
| 1. | Noninflammatory,
also known as secretory, which occurs when organisms multiply in the
bowel and produce a watery diarrhea either directly or via
elaboration of a true enterotoxin. There is no invasion of the gut mucosa and usually no systemic signs such as fever. Cholera, giardiasis, and viral diarrheas are examples. |
| 2. | Inflammatory, also known as invasive, which occurs when organisms invade the gut mucosa (usually distal small bowel or colon) and produce a bloody diarrhea and systemic signs. Salmonellosis, shigellosis, campylobacteriosis, and amebiasis are examples. |
| 3. | Penetrating, also known as systemic infection, which occurs when organisms penetrate the gut mucosa without disruption or extensive destruction and cause infection of multiple organs that is sometimes accompanied by diarrhea. Typhoid fever and hepatitis A are examples. Agents operating by this mechanism will not be covered specifically in this chapter. |
Specific diagnosis of the type of infectious diarrhea) is rarely attempted in sporadic, outpatient episodes because these are frequent, mild, self-limited, and usually treated with supportive measures regardless of the cause. Clinical symptoms cannot be used to reliably distinguish between causes, but in outbreaks the epidemiologic characteristics may suggest a probable etiology.
Risk Factors and High-Risk Groups
Risk factors for different infectious diarrheas include extremes of age, season, living conditions (type of housing, crowding, sanitation facilities, and quality and quantity of water sources), personal habits (handwashing, food handling, foods eaten), group exposures (nosocomial in hospitals and long-term care facilities, infants and toddlers in diapers or in day care and their caretakers, slaughterhouse workers), compromised immunity, low stomach acidity (achlorhydria, gastrectomy, antacids, other drugs), being a traveller, and having altered gut flora (antimicrobials).
The severity and duration of infectious diarrhea depend on the infectious agent, the inoculum, proper treatment with fluids to avoid dehydration, and host factors such as immune defenses and extremes of age.
The disability from infectious diarrhea is generally mild and short-lived, although some patients develop chronic diarrhea or other chronic sequelae.
Child Day-Care Centers
Children attending day-care centers are at increased risk of diarrheal disease from a variety of infectious agents compared with children who are cared for at home. Although many of these episodes are mild and self-limiting, they occur frequently, can be spread to other members of the child’s household, and may result in a significant loss of work for the child’s parents and a loss in household income.
Several factors contribute to the transmission of infectious diarrhea in the day-care setting. Children in day-care centers characteristically come into close physical contact with a number of other children, resulting in increased opportunity for respiratory droplet and aerosol transmission. In addition, infants and young toddlers typically have poor personal hygiene, are incontinent of feces, and frequently put their hands and other objects in their mouth. Young children also are immunologically susceptible to a variety of infectious organisms.
Bacterial Diarrheas
Salmonellosis
Salmonellosis is an infection caused by the Salmonella group of bacteria, other than Salmonella typhi.
Once swallowed, the organism must survive the gastric acid, and it begins to multiply on reaching the intestine. Within 12 to 72 hours after exposure, the typical patient develops abdominal cramps, diarrhea, and fever, which last 3 to 7 days in otherwise healthy persons. In high risk persons or in normal persons exposed to an extremely high dose, the organism can invade the bloodstream, spreading throughout the body and causing a profound illness.
Salmonella can cause infection in other organs, including the spinal cord, joints, or artificial blood vessels. After an infection, partial immunity develops so that a higher dose of that serotype is needed to cause symptoms. The infection does not appear to confer immunity to other serotypes.
The median duration of excretion of Salmonella organisms after infection is approximately 5 weeks.
Shigellosis
Shigellosis, or bacillary dysentery, is an infection of the intestine caused by bacteria of the Shigella genus.
Illness usually develops about 2 days after exposure but may occur within a few hours. Typical illness includes abdominal cramps, fever, and diarrhea that often is bloody. Illness usually lasts 1 week.
Infection with Shigella confers immunity to that serotype but not to other serotypes. No vaccine is available. Appropriate antimicrobial therapy decreases the duration of diarrhea, fever, abdominal pain, and excretion of Shigella in the stool. However, antimicrobial resistance has been a frequent and increasing problem with Shigella, and in many parts of the world, Shigella strains are resistant to all commonly used drugs.
E. Coli 0157:h7–Hemorrhagic Colitis
There are now five recognized classes of E. coli that cause diarrhea, each with a different virulence mechanism: enteropathogenic, enterotoxigenic, enteroinvasive, enterohemorrhagic, and enteroaggregative. Enterotoxigenic E. coli are an important cause of diarrhea in U.S. citizens traveling in developing areas. The enterohemorrhagic E. coli first were described in the 1980’s, and one serotype, E. coli 0157:H7, now is an important cause of bloody diarrhea and hemolytic uremic syndrome. The other classes of E. coli rarely cause illness in the United States.
Within 3 to 8 days after exposure to hemorrhagic E. coli the infected person develops severe abdominal cramps and diarrhea but usually no fever. In most reported cases, the diarrhea becomes extremely bloody within a day or two. The syndrome of grossly bloody diarrhea and severe abdominal pain in the absence of fever is called hemorrhagic colitis and easily may be confused with noninfectious diseases such as ulcerative colitis, Crohn’s disease, or ischemic colitis. Uncomplicated infections last 5 to 10 days and resolve spontaneously.
Hemolytic uremic syndrome, a serious illness characterized by anemia, thrombocytopenia, and renal failure, develops in 5 to 10 percent of persons with E. coli 0157:H7 infection. Evidence strongly suggests that E. coli 0157:H7 is the major cause of hemolytic uremic syndrome in the United States and that the frequency of this illness is increasing.
Viral Diarrheas
Viral diarrheas are noninflammatory diarrheas caused by a variety of viruses. The most frequently identified viruses include group A rotaviruses and Norwalk and Norwalk-like viruses. Less commonly identified uses include enteric adenoviruses, astroviruses, caliciviruses, and nongroup A rotaviruses.
There appear to be two general classes of viral diarrheas. One “endemic” type seems to infect all children at young ages regardless of sanitation; examples include group A rotavirus, calicivirus, adenovirus, and astrovirus. A second “epidemic” type seems to cause outbreaks related to poor sanitation. Modes of transmission are not known, but the former may occur through the respiratory route and the latter most commonly through the fecal-oral route or through contaminated vehicles such as food or water. Because viruses do not multiply outside their host, a contaminated common source with subsequent person-to-person spread is responsible for most outbreaks of viral gastroenteritis.
Preventing viral diarrheas is nearly impossible at present, so efforts have focused on preventing serious outcomes, such as dehydration and electrolyte imbalance, through adequate fluid replacement. Oral rehydration therapy is important in the United States and particularly in developing countries.