|
|
|
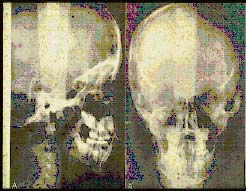
Figure 44. Lateral and frontal cephalometric radiographs |
|
|
|
Figure 44. Lateral and frontal cephalometric radiographs |
Although a discussion of cephalometrics is a course in itself, it is difficult to discuss growth and development without mentioning this important diagnostic tool. In 1931, Dr. B. H. Broadbent, an orthodontist, developed radiographic cephalometrics as a method to study the growth and development of the craniofacial complex. (13) (Figure 44) It later became the most important diagnostic tool for orthodontic treatment.
Most contemporary orthodontists use cephalometrics in performing growth forecasts of their patients. Short term growth forecasts, for periods up to 4 years, can be performed manually.(14) Computers are now used to perform long term growth forecasting for periods of 10 years and more.(15)
|
|
|
Figure 45. Growth of cranial base |
To give you some idea of how craniofacial growth takes place, the cranial base, a line depicted between "Basion" (anterior point of the foramen magnum) and "Nasion" (fronto-nasal suture) grows approximately 2mm per year during the active growth of an individual. (Figure 45)
|
|
|
Figure 46. Growth of mandibular corpus |
The "Corpus Axis," a line from a point above the chin on the outer surface of the mandibular symphysis to a point representing the center of the mandibular ramus also grows 2mm per year. (Figure 46) Therefore, there is a 1:1 ratio between the growth of the cranial base and the growth of the body of the mandible in a normal individual, as in a Class I situation. (Figure 47) In a Class II division 1 patient, this ratio may be in the range of 1:0.5, and in a Class III it may be as large as 1:3. Interestingly, research performed at the University of California, Los Angeles, found that Class II division 2 patients have a ratio of 1:1.5 and as great as 1:2 when the upper incisors are tipped forward and the bite opened.(16) This may be attributed to what is termed "rebound growth."
|
|
| Figure 47. Growth ratio of cranial base and mandible |
In other words, the mandible "catches-up" to its normal growth pattern in certain Class II division 2 patients, once the lower jaw is "unlocked" by the anterior deep dental bite. Oftentimes, a simple appliance such as a removable anterior bite plate can be utilized by the clinician to not only allow for the eruption of posterior teeth to open the bite, but also enable the mandible to follow its "morphogenetic" growth pattern.
The facial axis is a line from PT point (foramen rotundum of the sphenoid bone) to a point on the chin (GN or Gnathion on the mandibular symphysis). It grows an average of 3mm per year. (Figure 48) It forms an angle with the cranial base (Ba -N), and this is 90 degrees in a normal Class I patient. (Figure 49) In this situation, the mandible's growth is equal in its downward and forward direction. A small angle of less than 90 degrees indicates a more downward direction of mandibular growth.

|

|
| Figure 48. Growth of facial axis | Figure 49. Facial axis angle |
This is seen in Class II division 1 dolichofacial patients, and is not favorable for the self correction of the Class II malocclusion.
On the other hand, if the "facial axis angle" is greater than 90 degrees, it would indicate a more forward growing mandible. This is usually the case in Class III developing malocclusions, and often in Class II division 2 patients. The latter is an indication that in brachyfacial individuals, mandibular growth is favorable as far as the prognosis of the treatment of the Class II situation.
The term "differential diagnosis" was defined in an earlier chapter to be "the process whereby the dentist determines the degree of difficulty of the orthodontic problem." The clinician can then determine whether or not to treat a malocclusion or refer a difficult problem to an orthodontic specialist. There is not a better single criterion than the facial axis angle to determine the degree of difficulty of a malocclusion, especially in the growing child.
This is why it should behoove the general dentist to learn as much as he or she can about the art and science of cephalometric analysis. There are numerous research articles and textbooks available to learn this most important diagnostic tool. (17), (18), (19)
|
| Figure 50. Lower incisor relationship to APo line |
Another most important diagnostic cephalometric measurement for the general practitioner is the distance between the tip of the incisal edge of the lower central incisor and a line between the "apical base" of the maxilla (A point) and the tip of the chin (Pogonion or Po). (Figure 50) The latter line is called the "APo" line and is really the axillomandibular line, since it connects the upper and lower jaws.
In a normal Class I individual, this measurement should be +1mm. In other words, the mandibular central incisor should be 1mm ahead of the APo line. In various malocclusions, the lower incisor can be further forward as in a bimaxillary protrusion, or in cases of thumb sucking, it could be lingually positioned in reference to the APo line.
The position of the lower incisor in a labio-lingual direction is obviously going to effect arch length. Any movement of the lower incisor labially or lingually is going to effect the arch length by twice as much. In other words, if the lower incisor is +6 to the APo line, and it is tipped back to the normal +1, there is going to be a decrease of the arch length by 10mm. Other teeth would probably have to be extracted in order to accomplish this orthodontically. On the other hand, if the lower incisor needs to come forward 5mm, this will increase the arch length by 10mm, and the clinician would more than likely be able to treat the case without the extraction of teeth.
It is often said by orthodontic specialists that they would prefer utilizing cephalometric analyses to determine the degree of difficulty of a malocclusion, rather than just a set of study models of the teeth. This is contrary to the thought of many general dental practitioners who more often use only study models to try and determine the extent or seriousness of an orthodontic problem. Nonetheless, it can easily be seen after the above discussion of the importance of the relationship between the lower incisor and the APo cephalometric line that one must use cephalometrics, in conjunction with study models, in order to perform an accurate arch length-tooth mass analysis to determine the extent of crowding or spacing in a dental arch.
![]()
References
13. Broadbent BH, A new x-ray technique and its application to orthodontics, Angle Orthodontist, 1:45-66, 1931.
14. Ricketts RM, Bench RW, Gugino CF, Hilgers JJ, Schulhof RJ: Bioprogressive therapy, Denver, 1979, Rocky Mountain/ Orthodontics.
15. Ricketts RM, Bench RW, Hilgers JJ, An overview of computerized cephalometrics, American Journal of Orthodontics, 61:1-28, 1972.
16. Levy PC: A study of mandibular growth of Class II division 2 malocclusions, thesis, Los Angeles, 1979, University of California, Los Angeles Orthodontic Department.
17. Downs WB, Variations in facial relationships: their significance in treatment and prognosis, American Journal of Orthodontics, 34:812-840, 1948.
18. Riedel RR, The relation of maxillary structures to cranium in malocclusion and in normal occlusion, Angle Orthodontist, 22:142-145.1952.
19. Ricketts RM, Roth RH, Chaconas SJ, Schulhof RJ, Engel GA: Orthodontic diagnosis and planning, 2 vols., Denver, 1982, Rocky Mountain/Orthodontics.
![]()