| Contents | Previous | Next |
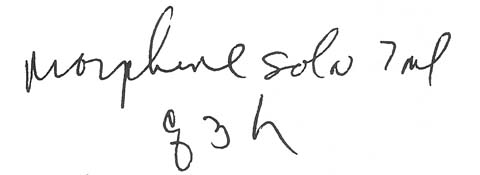
A medication nurse was given this order for a patient with cancer pain:
|
|
The nurse took a bottle of liquid morphine from the narcotics supply, poured out 7 ml, and administered it. Three hours later, she repeated the dose.
An hour after the second dose was given, the patient was found unconscious and barely breathing. Her skin was cold, pale, and moist. Suspecting a morphine overdose, her doctor ordered naloxone (Narcan). Three 0.25-mg doses had to be given before the patient revived.
Both the doctor and nurse wondered how two 14-mg doses of morphine could affect the patient so severely. The nurse decided to look more closely at the bottle of morphine she had used to obtain the dose. She was shocked when she read the label. The concentration of morphine was not 2 mg/ml, as she had thought, but 20 mg/ml. She had given the patient 280 mg of morphine.
The patient was lucky that her condition was discovered and treated promptly; such a high dose of morphine could have been fatal. This error happened because the nurse left out a basic but crucial step in medication administration-reading the label. She didn't know two concentrations of liquid morphine were available and simply poured the amount of milliliters ordered.
To prevent such an error, encourage doctors to write orders for liquid medications in milligrams rather than milliliters. Ask pharmacists to clearly indicate the concentrations of these drugs on their labels. And of course, always verify that you have the correct concentration when obtaining a liquid medication.