| Contents | Previous | Next |
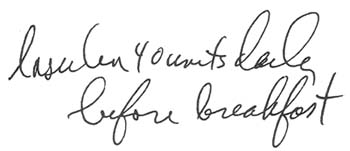
A doctor wrote the following order for an elderly insulin dependent woman:
|
|
Since he didn't specify the type of insulin, the nurse assumed it was regular insulin and noted that on the patient's medication administration record.
The patient was given 40 units of regular insulin for 2 days.
Before lunch on the second day, she developed signs of hypoglycemia. A stat blood glucose test revealed an abnormally low level of 40 mg/dl. She was immediately given a bolus of 50% dextrose injection, and her condition improved.
Both doctor and nurse were nonplussed by the patient's hypoglycemia. Trying to determine the cause, the nurse asked the doctor if he had increased the dose of regular insulin. The doctor replied, "Regular? I thought I ordered NPH."
The nurse then realized what had happened: When the doctor didn't specify the type of insulin on the order, she had assumed he wanted regular when, in fact, he wanted NPH. The patient's blood glucose level had dropped because she'd been given the fast-acting regular insulin instead of the slower-acting NPH. When the nurse explained what had happened, the doctor wrote a new order specifying NPH insulin.
To prevent similar errors, always question insulin orders that don't specify type of insulin. Also, as a rule of thumb, question any dose of regular insulin that's over 25 units. With the purified animal and human species insulin's available today, such a dose would be unusually high unless the patient had severe hyperglycemia or ketoacidosis.