| Contents | Previous | Next |
A 75-year-old man recovering from a cerebrovascular accident was hospitalized for treatment of a foot ulcer. Four days after his admission, the medication nurse prepared to give him his bedtime dose of thioridazine (Mellaril), an antipsychotic.
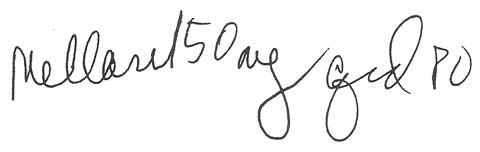
The nurse obtained the dose from the patient's bin in the drug cart and compared it with the order in his medication administration record (MAR). The order called for 50 mg, but the dose she'd taken from the bin was labeled 150 mg. Checking the doctor's original order, she read:
|
|
The nurse immediately realized that though the unit secretary had transcribed the order correctly, the pharmacist had misinterpreted it, seeing the I on the end of Mellaril as the numeral] before the 50. She called the pharmacist, who looked at his records and saw he had entered the order as 150 mg. He checked his copy of the original order and agreed he'd misinterpreted it.
The patient had received a threefold overdose of a major tranquilizer. Although he had become increasingly sedated, nobody had questioned why. Fortunately, he didn't develop more serious reactions to the drug.
This error occurred because the nurses giving the first three doses didn't check one of the five "rights" of drug administration-the right dose-when comparing the drug with the order in the MAR. Don't make the same error yourself. Every time you give a drug, know your rights: patient, drug, dose, time, and route.