| Contents | Previous | Next |
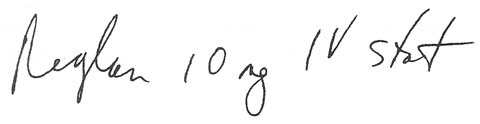
During a hectic day on an understaffed nursing unit, an inexperi¬enced nurse was given the following order for a patient who had diabetic gastroparesis:
|
|
The nurse called the pharmacy for the dose, and a pharmacist arrived almost immediately with a bag containing five ampules.
The nurse quickly checked the pharmacist's label on the bag. It read: metoclopramide (Reglan), 2 mg/ampule. 2 mg x5 ampules = 10 mg. Use all 5 ampules. She drew up and administered the contents of all five ampules by slow I.V. push.
Before discarding the empty ampules, the nurse checked the original label. She froze when she read 10 mg/2 ml. Obviously the pharmacist had confused 2 ml with 2 mg. As a result, the nurse had given 50 mg of Reglan.
The patient was closely observed for the next 8 hours, but he developed no ill effects from the overdose.
This error could have been prevented if the pharmacist had read the manufacturer's label more carefully and the nurse had checked it before giving the drug. Also, she should have asked herself why she'd been given five ampules for one dose. Generally, using more than two units to complete a dose signals a problem ..
When more than two ampules are needed for one I.V. dose, the drug is usually diluted. So giving five ampules I.V. push should have alerted the nurse that something was wrong.
To prevent a similar error: Do your own dose calculations. Scrutinize the manufacturer's label. Don't confuse ml and mg. And always check everything again when you need more than two of anything to complete a dose.