| Contents | Previous | Next |
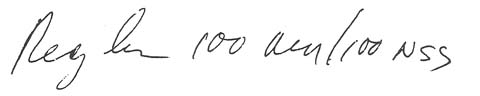
To prevent the nausea and vomiting associated with cancer chemotherapy, a doctor ordered 1 00 mg of I.V. metoclopramide (Reglan) for a patient who was to begin receiving cisplatin. The doctor wrote the order as follows:
|
|
The medication nurse, interpreting the order as "Reg In," administered 1 00 units of regular insulin to the patient. She thought the dose was unusually high, but because of an extremely busy schedule, she didn't question it.
When the nurse returned to the patient's room about 20 minutes later, she found him comatose. She called the doctor immediately and reported the patient's condition, adding that she'd given him the 100 units of regular insulin as ordered. The doctor answered that he'd ordered Reglan, not insulin, then instructed her to give the patient 1 mg of glucagon I.V. stat. The patient was given a second dose of glucagon about 25 minutes later and began to respond. He recovered within a few hours.
Several elements of bad practice led to this medication error. First, the order was carelessly written, causing it to be misinterpreted.
Second, the nurse didn't question the unclear handwriting. The dose was unusually high too. Any time you see a dose of regular insulin above 25 units, check it out to make sure it is correct. Today's purified animal and human species insulin don't usually warrant such a high dose.
To add to the possibility that these two drugs could be confused, metoclopramide is also indicated for diabetic patients suffering from delayed gastric emptying, which is caused by diabetic gastroparesis. Thus, a diabetic patient could conceivably have an order for either Reglan or regular insulin (or both). All the more reason to be alert for drug names that look alike.