| Contents | Previous | Next |
A 56-year-old diabetic woman was hospitalized for treatment of foot ulcers. During her admission interview, she stated that she took NPH insulin: 70 units at breakfast and 30 units at dinner.
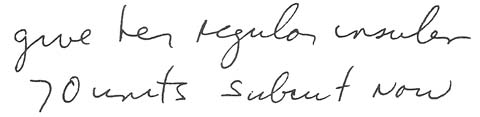
The morning after admission, the patient's breakfast and insulin were ordered held until some X-rays were taken. When she returned to her room, her doctor wrote the following order:
|
|
The nurse immediately administered 70 units of regular insulin to the patient, who then ate her breakfast.
A short tIme later, the patient said she felt dizzy. Her nurse called in the doctor, who asRed about the dose administered. When the nurse told him she'd given the ordered amount of 70 units of regular insulin, the doctor realized what had happened. He'd meant for the patient to have her usual insulindose, 70 units of NPH insulin.
The patient was immediately given orange juice, and she recovered from the insulin error without any further reactions.
Of course, the main cause of this error was the doctor's misleading order. But the nurse should have questioned a dose of 70 units of regular insulin for a patient who wasn't hyperglycemic. In fact, with the purified and human insulins available today, any time more than 25 units of regular insulin is needed for a single dose, the order should be questioned.
Medication errors with insulin are among the most common because insulin isn't ordered on a regular schedule as other drugs are. So be extra cautious: