| Contents | Previous | Next |
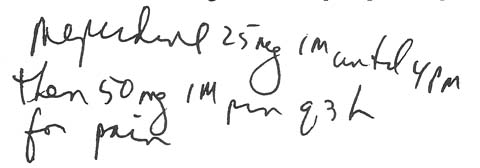
A doctor wrote the following order for a postoperative patient:
|
|
Attached to the patient's chart was a sticker saying he'd received the anesthetic Innovar before his surgery.
At 3 p.m., the patient complained of pain. The medication nurse checked his medication administration record, obtained what she thought was the correct analgesic from the unit-dose narcotic floor stock, and administered it.
Moments later, the charge nurse checked the meperidine con¬trol form and noticed the medication nurse hadn't signed out any doses. When questioned, the medication nurse insisted she'd signed the form. When she produced the form, the charge nurse saw it was for morphine. The medication nurse had mistakenly read morphine for meperidine.
The usual dose of morphine is 10 to 12 mg. But when the patient has received Innovar, the morphine should be reduced to 4 mg. This is because the patient still had some anesthetic in his blood, and certain anesthetics, including Innovar, contain narcotics. So if the narcotic analgesic dose isn't reduced, this dose on top of the anesthetic's narcotic could be high enough to cause respiratory depression.
Since this patient had received about six times the safe dose of morphine, he developed respiratory distress and had to be given a narcotic antagonist to counteract the overdose.
This medication error could have been avoided if the medication nurse had carefully read the order. She also should have known a dose of 25 mg of morphine is too high for any patient. Further, she should have double-checked the dose when she saw the warning sticker on the patient's chart.
If you administer narcotics to postoperative patients, you should know about their dangerous additive effects on anesthetics. Always check to see what anesthetics a patient received, read all warning stickers, and question anything that seems out of order. Your extra caution could save a patient's life.