| Contents | Previous | Next |
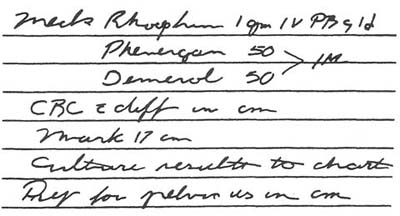
A pharmacist received this medication order:
|
|
Following standard procedure, the nurse who'd processed the doctor's order had also sent the pharmacist a copy of her transcription. In the section of the medication administration record (MAR) marked "orders," she'd incorrectly noted the frequency for the antibiotic Rocephin (which she-and the doctor-had spelled Rhocephin) as "q.i.d." The pharmacist called her immediately and told her to change the MAR entry to "q12h" before an error was made. Rocephin is normally given only once or twice a day.
This transcription error is a good example of how illegible handwriting causes problems and why at least two professionals-a nurse and a pharmacist-must interpret every drug order. Here, the nurse had misread the doctor's sloppily written "q12h" as "q.i.d." Plus, he'd spelled the drug's name incorrectly and she'd copied it that way. And because she hadn't suspected an error, she didn't consult the unit's drug handbook.
At some hospitals, only one person interprets orders. For example, the nurse may forward a transcription of the order-but not the original order-to the pharmacy. This most often occurs in critical care areas of the hospital, such as the operating room, emergency department, and intensive care unit. So the pharmacist won't necessarily know if she's made an error. Similarly, a problem might come up if a nurse doesn't double-check the pharmacist's work when he interprets the order and prepares a computerized MAR.
Luckily, the pharmacist caught this transcription error before the patient received twice the prescribed amount of Rocephin. That underscores the value of the nurse and pharmacist doublechecking the original order.