| Contents | Previous | Next |
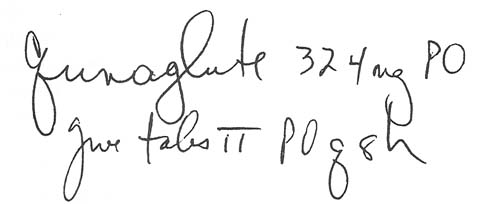
A patient hospitalized for fainting spells was found to have frequent premature ventricular contractions. Her doctor ordered two tablets of quinidine gluconate (Quinaglute), an antiarrhythmic, given every 8 hours. Quinaglute is available only in 324-mg tablets. So the nurse who transcribed the order onto the patient's medication administration record (MAR) wrote it this way:
|
|
During the night shift, the medication nurse prepared to administer this patient's drugs. She glanced at the MAR and saw "Quinaglute, 324 mg." Thinking just one tablet was called for, she pulled apart the two unit -dose packages that had been taped together by the pharmacist and used only one of them. The pharmacist discovered the error in the morning when he found the leftover tablet in the patient's drug bin.
This error could have been prevented if the nurse transcribing the order had clearly stated two tablets were needed: Quinaglute, 648 mg (2 x 324-mg tablets), q8h. Also, the medication nurse should have stopped to consider why the two packages were taped together. Most pharmacists using a unit-dose system will do this (or leave the packages unperforated) when an order requires more than one dose unit.