| Contents | Previous | Next |
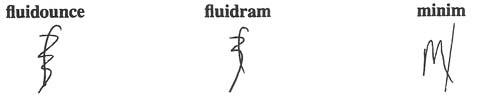
A woman with a history of peptic ulcer disease was admitted to a long-term care facility. Her doctor ordered Maalox, 30 ml,, 1 hour before meals and at bedtime. The nurse who transcribed the order used the apothecary symbol for fluidounce (see below)-or so she thought. What she actually used was the symbol for fluidram (see below), which is equivalent to 5 ml. Consequently, the patient was given only 5-ml doses for several days. The error was discovered when another nurse questioned the low dose.
Granted, this is not an earthshaking medication error. But think what could have happened had the order been for oral theophylline, morphine, or cyclosporine. The patient could have been dangerously undermedicated. Or consider the consequences if the symbol for ounce had been written for dram: The patient would have received an overdose.
The apothecary system of measurement has long outlived its usefulness. It's confusing and hazardous. Many doctors and nurses interchange the abbreviations for ounce and dram in drug orders. They mistake the designation minim (see below) for ml.. And they confuse grains and grams.
Yet some nursing schools still teach the apothecary system. Doctors persist in using it in their orders. Even drug companies promote its use. A minim scale still appears on some syringes, and doses in grains remain on some manufacturers' labels (for example, labels for sublingual nitroglycerin tablets).
Don't let the apothecary system put your patients at risk. Discourage its use whenever you can. For drug doses, metric is the only way to go.
|
|