| Contents | Previous | Next |
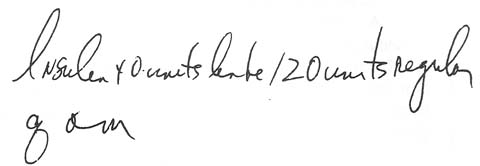
A nurse, following a doctor's written order, gave her diabetic patient 40 units of lente insulin with 120 units of regular insulin. A short while later, she realized the patient was showing signs of an insulin reaction. She called the pharmacist, told him what she'd administered, and asked him to check the original order. It looked like this:
|
|
The pharmacist interpreted the order as 40 units of lente insulin with 20 units of regular insulin. He realized at once what the nurse had done-she'd read the slash before the 20 as a "1." As a result, she'd given an insulin overdose.
The nurse alerted the patient's doctor, who ordered a stat blood glucose test. As suspected, the patient was hypoglycemic. Several doses of I.V. glucose were needed to bring her glucose level back to normal.
A doctor's shorthand-. -using a slash instead of writing out "with" -caused the nurse to misinterpret his order. Regrettably, she didn't stop to consider that 120 units of regular insulin was an unusually large dose.
Don't let medication administration become a mindless process. Think an order through before you carry it out. And watch for those slashes that could be mistaken for a "1."