1. Infectious Disease Defenses
A. Natural Resistance
1. Skin as a boundary
2. Mucous membranes
A. Eyes/ears
B. Respiratory tract
C. Gastrointestinal tract
D. Genitourinary tract
3. Normal bacterial flora
4. Antimicrobial substances
A. Lysozymes
B. Interferon
C. Chemical mediators
D. Complement 5.
Phagocytosis
A. Chemotaxis
B. Engulfment
C. Killing and exocytosis B.
Internal Defenses: The Immune System
A. Primary Organs
1. Bone marrow
2. Thymus
B. Secondary lymphoid tissue
1. Lymph system (lymph vessels and lymph nodes
2. Spleen
2. Cells of the immune system C. The Immune
Response D.
Immunodeficiency
1.
Organs of the Immune System (Lymphoid System)
A. Hematopoiesis
B. Nonlymphoid cells
1. Monocytes and Macrophages
2. Granulocytes
3. Lymphoid cells
C. Lymphocytes
1. B-Lymphocytes
2. T-lymphocytes
1. Antigen Processing
A. Role of macrophages
B. Interaction of macrophages and Lymphocytes
2. B-lymphocytes - Humoral Immunity
A. Primary vs. Secondary antibody response
B. Antibodycomposition andfimetion
3. T-lymphocytes - Cellular Immunity
A. TH Iymphocytes
B. TK,TNK, and TS Lymphocytes
4.
Acquired Immunity
A. Natural
B. Artificial
5. Passive
immunity
A. Natural
B. Artificial
1. Congenital
immunodefficiencies
2. Acquired
immunodeficiencies - AIDS
Introduction
The development of immunology, the science of the immune system, began with the study of resistance or immunity (L. immunitas, freedom from) against infection. The seminal idea of acquired immunity is not recorded in history but must have existed long ago in the common knowledge that individuals who had recovered from certain childhood diseases, such as chickenpox, or epidemic diseases, such as smallpox, rarely developed that same disease again.
The recognition that dairymaids who previously had cowpox (vaccinia) were protected against epidemic smallpox was empirically applied in the 18th century by Edward Jenner (1749-1823), an English country doctor, who introduced the procedure of inoculating ("vaccinating") subjects with the infectious material of cowpox as a protection against smallpox. This stroke of genius, which opened the door of inquiry into what has become the sciences of immunology, virology, and preventive medicine, preceded by nearly a century the establishment by Louis Pasteur (1822-1895), eminent French chemist and bacteriologist, of the germ theory of disease and his development of vaccines of "attenuated" microorganisms for immunization against specific infectious diseases of domestic animals and man. Incredulous as it may seem today, the first report of Jenner's work, which was the culmination of 20 years of effort, was rejected for publication by the Royal Society as incomplete and unconvincing ("so much at variance with established knowledge, and withal so incredible"). Now, two centuries later and following a WHO (World Health Organization) global program of vaccination and isolation, small pox for all practical purposes has been eliminated from the earth.
In the late 19th and early 20th century, fundamental advances were made in understanding inate (natural) and adaptive (specific) immunity. The natural ability of phagocytic leukocytes to ingest and destroy bacteria was discovered. Specific "antibodies" which neutralized bacterial toxins were produced by immunizing animals with the appropriate bacterial "antigens". The humoral (antibody) immune response in animals sensitized against bacteria or other foreign antigens was characterized by specificity (ability to recognize one antigen and to distinguish it from another) and memory (accelerated response). The cellular immune response to the tubercle bacillus was recognized soon after the discovery of this bacillus. Serum complement, a major humoral component of inate immunity and mediator of inflammation, was discovered. The antibacterial phagocytic activity of leukocytes was shown to increase when specific antibody ("opsonins") and complement were both bound to the surface of bacteria, thus affording the host the double advantage of inate and adaptive immunity. Adverse, even life-threatening, immune reactions (hypersensitivity/ allergy) were also early recognized in sensitized animals and humans: anaphylaxis, serum sickness (attributed to "toxic complexes"), and delayed hypersensitivity (cell-mediated immunity).
The latter half of the 20th century produced further advances in the biology and pathology of the immune system: characterization of the cellular components and the central role of T and B lymphocytes; molecular structure of immunoglobulins, T cell receptors, and MHC molecules which recognize antigens; humoral and cellular mechanisms of tissue injury; immune tolerance (unresponsiveness to self); autoimmunity; transplantation immunity; tumor immunity; and immune deficiency.
The antibody- and cell-mediated immune responses protect vertebrate animals from myriads of infectious microorganisms-bacteria, viruses, fungi, and parasites- by targeting microbial agents as foreign and, aided by phagocytes and other components of inate immunity, destroying them. Also, the immune system preserves the "uniqueness" of the individual: it rejects transplants of histoincompatible cells and affords some "surveillance" of neoplastic cells.
A fundamental aspect of the immune response is the ability to distinguish foreign molecules from self molecules. For, as will be noted subsequently, a failure of "self-nonself" discrimination can lead to a destructive autoimmune response against one's own body tissues.
Thus, there are two edges to the "sword" of immunity: host protection and injury. Disorders of the immune system- hypersensitivity, autoimmunity, and immune deficiency- produce a wide range of clinical conditions of common or rare occurrence. Many local and systemic diseases, some of them life threatening, are caused by overly active or misdirected immune reactions, that is, by hypersensitivity or autoimmune mechanisms. Immune deficiencies also take a large toll of life. Severe immune deficiency imposes a high risk of death from opportunistic infection or malignant neoplastic disease, such as occur in AIDS (acquired immune deficiency syndrome) which is caused by HIV (human immunodeficiency virus) infection and is now becoming a global epidemic.
Courtesy
of Robert C. Mellors, M.D., Pd.D.
http://edcenter.med.cornell.edu/CUMC
Reprinted with
permission.
Natural resistance or innate immunity refers to a broad group of mechanisms and factors that we are born with and that are often unique to a species. This innate immunity provides us with a general barrier to infection rather than a specific resistance to a particular agent or organism. Innate immunity is said to be non-specific. The normal bacteria that live within us and on us are an important part of this non-specific immunity. These organisms produce substances that work as antibiotics and often suppress the growth of more hazardous organisms. For this reason, the unnecessary use of prescription antibiotics can be detrimental to health.
The skin is the largest organ of our body and is a critical component of our innate immunity. Skin is a physical barrier that blocks most organisms from entering our body. Many organisms attempt to penetrate skin; they attach and begin to grow. However, their efforts are usually thwarted by the normal shedding of our outermost layer of skin. Additionally, sebaceous glands near hair follicles which cover most of our body produce oils that have an anti-fungal effect. Because the palms of the hands and the soles of the feet lack hair, and therefore sebaceous glands, they are the sites that are most susceptible to fungus infections.
The "portals of entry" into our body include such areas as the eyes, respiratory track, digestive track and genital-urinary track. These sites offer an opportunity for infection and penetration of the human body and therefore are well-endowed with innate immunity. The small hairs that line the respiratory tract, called cilia, wave upward, continuously pushing anything that enters the throat back toward the mouth. When these infectious agents and other particles enter the respiratory track, they are coated with mucous secretions, pushed upward by respiration and ciliary waves until they reach the cough reflex tissue near the epiglottis. Once there, they trigger the cough reflex resulting in such particles either being expelled from the body or swallowed. If swallowed, these particles then enter the digestive tract.
The digestive tract is an exceedingly difficult route for an infectious agent. The high acidity of the stomach is equivalent to concentrated hydrochloric acid. Then the high alkalinity of the small intestine is as caustic as Iye. Few, if any, infectious agents can survive this acid/alkali treatment. If that were not enough, the enzymes used for digestion continuously act on organic substances breaking them down to biochemical nutrients.
The genital/urinary tract is equally well protected. The physical structure of these organs, together with the mechanical flushing that occurs in urination and defecation, as well as during the female menstrual flow, provide a superb means to prevent infection.
Many substances are produced in our bodies that have an antimicrobial effect. For example, an enzyme called Iysozyme is present in tears, saliva and other mucous secretions. This enzyme is capable of destroying bacterial cell walls. Another group of molecules, called interferons, are produced by all human nucleated cells. These molecules serve a number of functions, including production of anticancer and antivirus effects.
The complement system is a large group of proteins that are activated in infection. When activated, complement factors result in the formation of molecules that can puncture cell membranes and, while doing so, increase blood flow and attract more white blood cells.
One of the most important components of innate immunity is the phagocytes, cells capable of engulfing foreign substances. Examples of phagocytes are the polymorphonuclear leukocyte and the macrophage-monocyte. These cells have the ability to move toward the site of infection, actively to seek infectious agents, and to engulf them. Once phagocytized, the infectious agent is packaged by the cell into a vacuole called the phagolysozome. The phagocyte then releases enzymes and toxic substances that have high levels of acidity. This environment kills most infectious agents.
In addition to physical mechanisms, such as the mechanical clearing of the eyes through blinking, or expulsion of foreign material through sneezing or coughing, innate immunity is also composed of such physical phenomena as body temperature. Each organism lives within a precise temperature range. Those that cause human disease grow well at 37 degree centigrade or 98.6 degree fahernheit. Any variation from that ideal temperature causes either a marked die off of the pathogens or at least a condition in which they fail to thrive. This is the reason that the body produces an elevation of temperature, in the form of a fever, when an organism has successfully initiated an infectious process.
Innate immunity is an important part of our natural defenses that assist us in our efforts to survive. As a species we are born with our innate immunity, and it remains relatively stable throughout our life. These mechanisms are entirely different from those that are included in our acquired immunity.
Immunology is the study of the immune system and the immune response, or the study of how the body protects itself from infectious disease. In immunology we study the organs and cells of the immune system and the way in which these function to protect us from the many harmful organisms in our environment.
What are the organs and tissues of the immune system?
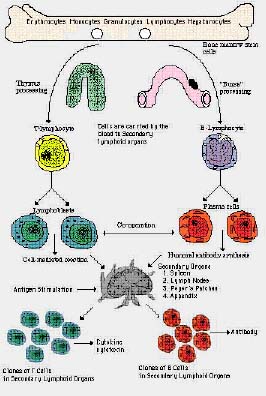
The primary organs of the immune system are the bone marrow (located within the bone) and the thymus (located in the chest above the heart). These organs are significant because they are the site of the production and maturation of the most important cells of the immune response: the Lymphocytes.
The thymus is composed primarily of Iymphocytes and epithelial cells and is connected to the Lymphatic system. The Iymphatics along with the spleen make up what is referred to as the secondary Iymphoid tissue.The Iymphatic system is a network of vessels throughout the body which circulate Iymph fluid. This fluid contains cells and proteins (Iymphocytes and antibodies) of the immune system which bathes tissues and organs in a protective medium. These vessels form nodes in the neck, axilla and the groin. Lymph nodes filter lymph fluid and trap microorganisms. These trapped invaders stimulate lymphocytes to mount a defense against them, the outward sign of which is seen as swollen Iymph nodes (swollen glands). The spleen is an abdominal organ located just below the rib cage. The Iymphocytes present here defend the body against blood-borne microorganisms.
What are antibody and complement molecules and what are their functions?
Proteins present in the serum can be classified as either albumins or globulins. A portion of the globular fraction of serum is referred to as immunoglobulins, globulins having immune properties. This group of proteins include antibodies which react with foreign substances, called antigens, which lead to destruction of antigens. A second group of proteins is referred to as the complement system, and activation of this system by antigen-antibody complex leads to active protein which can destroy the antigen and attract immune cells.
What are the cells of the immune system?
Before discussing specific cell types and their role in the immune response we should first discuss hematopoiesis. Cells of the blood are produced in the bone marrow and this process is referred to as hematopoiesis [Gr. haimatos, blood, + poien, to form]. All blood cells originate from a common precursor cell called a stem cell. The stem cell is capable of self-renewal by producing daughter cells through mitosis (cell division) and it can also differentiate into different blood cell types. Blood cells are generally classified as red blood cells (erythrocytes) or white blood cells (leukocytes). Red blood cells contain hemoglobin and are responsible for transporting oxygen from the lungs to the tissues. There are many different types of white blood cells, and each of these plays a role in protecting us against infectious disease.
The cells of the immune system are white blood cells, and these can be categorized as either Lymphoid cells or non-lymphoid cells depending on whether or not they reside predominantly in the network of vessels, nodes and organs that comprise the Lymphoid system.
Lymphocytes (Iymphoid cells) are round, mononuclear cells, motile but non-phagocytic and range in size from 6 to 14um. They comprise approximately 25-40% of the circulating white blood cell population. They can be classified as small or large, inactive or active, long-lived or short-lived. Small Iymphocytes in the 6-8um range are relatively inactive and may be able to live for years. When stimulated, small Iymphocytes undergo blastogenesis and are transformed into large Iymphocytes which are capable of dividing, thus increasing the cell population. Antigen (def: any substance recognized as foreign that can cause an immune response, i.e., proteins microorganisms are made of) is the natural stimulus that induces blast transformation and cell division. Antigen stimulated lymphocytes either react directly with the antigen or produce immunoglobulins (antibodies) which react with the antigen.
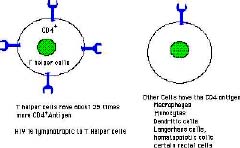
There are two subsets of Iymphocytes which are responsible for what is referred to as the "duality of the immune response." These cells differ in their maturational origin and in the way they interact with antigen. B-lymphocytes mature in the bone marrow and upon antigen stimulation these cells become antibody secreting plasma cells. Antibodies (immunoglobulin proteins) circulate in the blood and bathe organs, tissues and cells in a protective solution and can bind to antigen rendering it inactive or label it for destruction by other cells or complement. B-lymphocytes are thus responsible for humoral Immunity. Lymphocytes, on the other hand, mature in the thymus and interact with antigen on a cellular level.T-cells are lymphocytes that bind directly with antigen and are then stimulated to divide. T-lymphocytes are therefore responsible for cell-mediated Immunity. T-lymphocytes are further divided into T-helper, T-suppressor, T-cytotoxic and T- delayed hypersensitivity cells depending on their specific function.
Non-lymphoid white blood cells that participate in the immune response include monocytes and macrophages, and granulocytes (neutrophils, eosinophils and basophils). Monocytes and macrophages are large (12-18um) mononuclear cells which are capable of phagocytosis. Phagocytosis is a process of seeking out and engulfing material for the purpose of destroying it. Monocytes carry out this function in the blood, and macrophages guard the tissues. Surface receptors on these cells confer a degree of specificity to their phagocytosis. These cells also play a critical role in antigen processing that allows Iymphocytes to respond maximally to antigen. Granulocytes have a lobulated nucleus, granular cytoplasm and are 10-15um in size. These cells are also capable of phagocytosis. Their cytoplasmic granules are rich in enzymes that digest phagocytized organisms.
Neutrophils are the body's main line of defense against bacteria. Chemicals released by bacteria or antibody-activated complement direct these cells to the site of infection. Eosinophils attack infectious agents that are too large to be engulfed by a single cell, i.e., parasites such as protozoa and worms. Basoophils are involved in the response to allergens.
 A few years ago a valiant young
man made history before he died. David, "the bubble boy," had lived for more than twelve
years with no immunity. Because he lacked immunity, he could only eat processed sterilized food, he
could not touch another human without the protection of gloves, and he lived in a National Air and
Space Agency controlled environment bubble. Even birth had to be in a totally germ-free environment
and was accomplished through a Cesarean section. Indeed, David's life was a miracle, and his death
has resulted in an enormous wealth of information that will help others born with his affliction,
congenital immunodeficiency. While David's story is a dramatic one, it is a story that, with a few
modifications, is being repeated thousands of times. For while David was born without immunity,
people with AIDS acquire a failure in immunity.
A few years ago a valiant young
man made history before he died. David, "the bubble boy," had lived for more than twelve
years with no immunity. Because he lacked immunity, he could only eat processed sterilized food, he
could not touch another human without the protection of gloves, and he lived in a National Air and
Space Agency controlled environment bubble. Even birth had to be in a totally germ-free environment
and was accomplished through a Cesarean section. Indeed, David's life was a miracle, and his death
has resulted in an enormous wealth of information that will help others born with his affliction,
congenital immunodeficiency. While David's story is a dramatic one, it is a story that, with a few
modifications, is being repeated thousands of times. For while David was born without immunity,
people with AIDS acquire a failure in immunity.The immune system has evolved to protect us from the environment around us. The world is full of microorganisms and toxic agents that would quickly destroy us if it were not for our immunity. The human immune system is an astonishingly coordinated response that is able to identify all that is self and all that is foreign and proceeds to eliminate that which is foreign. The cells and proteins of immunity can attack organisms that are free living within us or those that live within our cells, as intracellular parasites. In a way, each immune response is an evolutionary response at the cellular level that produces a unique immunity against a new organism.
Many microorganisms live in a parasitic relationship with higher animals such as humans and require our existence to support their life. A natural outcome of the principle of parasitism is that the death of a host is disadvantageous to the parasite. In many cases we have evolved to take advantage of this parasitic relationship. For example, certain intestinal bacteria produce substances that are necessary for digestion, immunity to other organisms, and the production of certain blood clotting factors.
Evolutionary change is a ubiquitous phenomenon. Each organism, whether human or bacteria, is in a constant process of responding and adapting to its environment. Certain environmental conditions offer an advantage to variants within a species which result in evolutionary change in the population. The short life span of microorganisms and the enormous diversity within a species result in an ability to change more rapidly. For this reason, microorganisms can evolve to become resistant to an antibiotic, and an organism that has never been a human parasite or pathogen may evolve to infect the human population successfully, as did the virus that causes AIDS. It should be clear that in this evolutionary race the microorganisms have the advantage, and some would say that we inevitably will be the loser of this biological struggle.
To overcome the problems associated with infectious disease, evolution has provided animals with a miraculous immune system. During each new exposure to a potential pathogen the cells of the immune system evolve to produce a specific immune response that can identify and destroy most infectious agents. This acquired immunity is crucial in the maintenance of life and is complemented by other factors in our resistance to disease. Acquired immunity is a learned response, and we are born only with the ability to develop acquired immunity. Each exposure to infectious agents results in cellular changes that lead to the development of effective immune responses to that organism. Here lie the two most significant differences between innate immunity and acquired immunity.
Acquired immunity is specific to a particular organism, and it is learned with exposure to that organism. Each exposure to an infectious agent improves the responses to that agent and each exposure to different agents expands the protection. For these reasons, infection in childhood serves an important role. Infection equips us with immunity that often lasts a lifetime. This is referred to as active immunity.
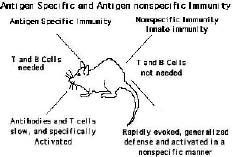
The immune response is an involved process by which the body defends itself against infectious agents. As we have already seen, there are several different white blood cells and proteins which play a role in the immune response. In order to understand fully the function of each of these and the way they work together to defend us, we must consider the three main characteristics of the immune response: recognition, specificity and memory.
Immunocompetent cells are able to recognize foreign antigen and differentiate it from self antigen. Receptors present on the surface of a Iymphocyte enable it to bind to antigen. It is the presence of these receptors which give specificity to the immune response. Each Iymphocyte can bind to and react with only a small number of specific antigens. If the cell recognizes the antigen as being foreign, the cell is activated to divide and differentiate. This results in a large number of identical Iymphocytes (clones) that specifically react with the antigen that stimulated their production. B-lymphocytes have surface immunoglobulin (slg) which bind to antigen. Activated B-cells differentiate into plasma cells which produce and secrete large amounts of antibody protein which can bind to and inactivate or cause the destruction of the antigen that stimulated their production. HLA-DR receptors on B cells allow them to interact with T-helper (Th) Iymphocytes. The exact mechanism of this interaction is not fully understood but B- cell/Tcell interaction is necessary to produce a maximal immune response.
 |
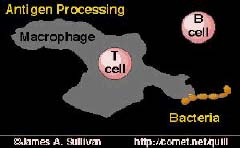 |
When Th-Iymphocyte bind to antigen they do it through the assistance of macrophages. Macrophages have surface receptors that bind to antigen. The antigen is phagocytized and degraded and then specific antigenic determinants are displayed on the macrophage surface. Activation of Th cells occurs when antigen is "presented" to the Th cell by a macrophage which has additional receptors on its surface which complement receptors present on the Th cell. Th cells cannot bind to antigen without binding to the antigen presenting macrophage as well. Activated Th cells release chemical substances which cause the proliferation of another type of T cell: the T-cytotoxic (Tc ) cell. Tc- Iymp-hocytes bind to cells that are infected with intracellular organisms such as viruses by binding to viral antigens displayed on the cell surface. Tc cells recognize the foreign viral antigens and destroy the cell in order to destroy the virus. A third type of T Iymphocyte involved in the immune response is the T-suppressor (Ts) cell. This cell has a regulatory function which serves to keep the immune response in check. Ts cells monitor the levels of antibody and antigen present and send out chemical signals to B and T Iymphocytes to stop proliferating when the threat of infection is over.
Initial exposure to an infectious agent produces an immune response which involves B Iymphocyte proliferation into antibody secreting plasma cells (humoral immunity) and T Iymphocyte proliferation of T-helper, cytotoxic and suppressor cells (cellular immunity). But the immune response would not be complete without immunologic memory: the ability of the immune system to remember an antigen which it has previously come into contact with. Immunologic memory allows the immune system to recognize an antigen it has seen before and respond to it much quicker and on a greater scale upon subsequent exposure. For example, upon initial exposure to a foreign antigen, B Iymphocytes differentiate into plasma cells and produce a primary antibody response to the antigen. Primary antibody only begins to be secreted after 3-4 days and it has a low level of specificity, i.e., is not all directed against the same portion of the antigen. The initial response is more concerned with producing a "weapon" as soon as possible and will worry about improving the effectiveness of that weapon later. If secondary exposure to that same antigen occurs months or years later, immunologic memory allows B "memory" cells to mount a secondary antibody response. Re-exposure to the antigen causes specific antibody to be produced more rapidly and in larger quantity. T "memory" Iymphocytes also circulate ready to defend against repeat offenders.
The heart of the learned response in acquired immunity is the selection of specific T- and B-cells that are capable of immune response to a particular agent. Repeated exposure results in expansion of that cell's producing a larger and larger clone. Initial contact with a microorganism may lead to infection and the development of acquired immunity; unfortunately, we often become ill and also develop the full spectrum of symptoms that typically describe a clinical syndrome. For example, in a streptococcal throat infection there are physical signs such as redness, swollen glands, and fever as well as the pain that is characteristic of a strep throat.
We may also develop consequences of that infection that may be more dangerous than the original illness, such as rheumatic fever or kidney disease. Another example that is of significance to college age individuals is measles. Measles has a characteristic syndrome that includes rash and fever which may reach extraordinary and dangerous levels in adults. Measles itself has a significant mortality rate in adults; additionally, measles during pregnancy may lead to birth defects and even the death of the fetus. For these reasons exposure to infection may not be the ideal way to develop immunity.
Modern medicine has given us one of the most important tools of health care today, that is, vaccination. Vaccination or immunization is a way of providing the individual with a form of the infectious agent that leads to the development of acquired immunity but does not lead to the infectious syndrome of the organism. This artificial form of immunization provides the individual with lasting immunity without the hazards of the disease and, along with antibiotics are probably the most important medical advance made in the history of humanity.
Through the use of immunizations, vast epidemics of polio, diphtheria, smallpox, whooping cough, and rubella have become occurrences of the past. Vaccines used in the immunization process are generally devised in the laboratory. Scientists usually take the organism that causes disease and treat it in a manner that makes the organism less viable and therefore incapable of causing disease. In some cases, killed organisms are used in immunization; in others, attenuated live viruses are used. Newer polio vaccines are good examples of attenuated organisms. These oral vaccines contain live polio virus that is able to cause local infection but unable to cause real disease. By staying alive for a period of time the virus is able to induce a more natural and permanent immunity.
Many look to immunization as the only real way that we can fully halt the AIDS epidemic. However, a number of major obstacles exist in the development of an AIDS vaccine. The HIV virus, because of its mode of replication, has a high degree of mutation inherent in its reproduction and produces numerous variants of itself. This trait is known as antigenic drift. There are reports of as many as 100 variants existing in a single individual. Any material used in a vaccine would have to identify a component of the virus that is stable.
The HIV virus is a lethal virus that only infects humans. This means that any trial with a vaccine would have to be done on humans and may involve the use of a lethal virus. Few volunteers can be expected for such an experiment. Moreover, suppose that a potential vaccine were discovered today; how long would it take to prove that it works? With an incubation period of up to 10 or 15 years, the results would not be complete until well into the 21st Century.
The most exciting advance in the development of a vaccine comes to us through recombinant DNA technology. Researchers may be able to synthesize subcomponents of the virus to use in vaccines without using the whole virus or prepare specific viral genes and insert them into a carrier organism for use in immunization. Currently, trials using such vaccines on people with AIDS are underway in an effort to induce a protective immunity.
Another form of acquired immunity is one called passive immunity. In passive immunity an immune state is acquired through another individual. A mother transfers through the placenta and through her milk immunity to the unborn and newborn infant. The use of gamma globulin shots is another way in which immunity can be transferred. However, passive immunity is temporary and lasts for a minimal period. Since it is not learned by the immune cells, it cannot be recalled as would acquired immunity.