|
|
|
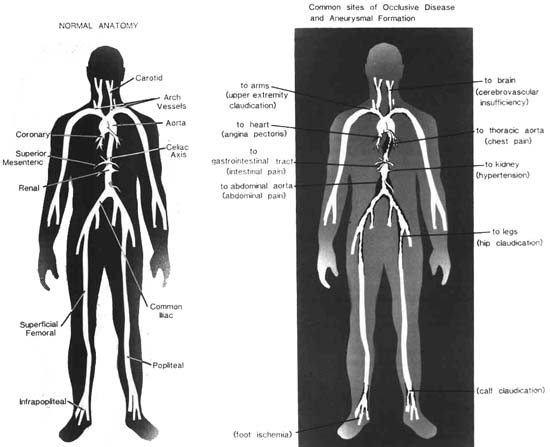
Figure 8.1 Common sites of occlusive disease and aneuysm formation. |
| Contents | Previous | Next |
Peripheral Arteriosclerosis
Peripheral arteriosclerosis is a major clinical problem. It involves the terminal portion of the abdominal aorta, the popliteal and iliofemoral arteries, and the below-the-knees arteries (Fig. 8.1). Frequently, the intimal layer of an artery is lined with atheromatous plaque but remains patent, so peripheral arteriosclerosis in these vessels goes undiagnosed in early stages.
People with diabetes mellitus are at high risk to develop peripheral arteriosclerosis. In fact, diabetes mellitus is the most prominent associated finding in patients with peripheral arteriosclerosis. Patients with femoropopliteal disease are also frequently diabetic, and aortoiliac disease is associated with diabetes, but to a somewhat lesser degree.
Hyperlipidemia is the second major etiologic factor. Many patients under age 50 with peripheral artery disease have some form of hyperlipidemia.
Cigarette smoking is another important etiologic risk factor. Studies have confirmed a relationship between smoking and arteriosclerosis in coronary, cerebral, and peripheral vessels. The effects on the peripheral vasculature are numerous. Tobacco accelerates the arteriosclerotic process through as yet unknown processes. There is some evidence that carboxyhemoglobin may injure the arterial intima. Nicotine is a known peripheral vasoconstrictor, further compromising blood flow in an ischemic limb. Also, smoking may accelerate platelet aggregation and cause an increased tendency to thrombosis.
Hypertension seems to potentate other risk factors such as diabetes and lipid abnormalities.
|
|
|
Figure 8.1 Common sites of occlusive disease and aneuysm formation. |
Polycythemia is another risk factor. As viscosity (the red cell mass) rises, it causes increased injury to the intimal lining of blood vessels. Intimal injury gives atherosclerosis an entry. This accounts for the propensity of atheromas to form at sharply angulated branch points in the arterial tree.
The pathophysiology of arterial occlusive dys function is thought to result from atherosclerotic, thrombotic, or embolic disease. Thrombosis refers to the formation of a blood clot in either the venous or arterial vasculature. An embolus is a detached thrombus and can consist of blood, air, or fat floating in the bloodstream until it becomes lodged in a smaller branch of the vasculature, creating an occlusion. Emboli occurring in the arterial system frequently have origins in the left heart. Atrial fibrillation and mitral valve stenosis are leading causes of atrial thrombi.
Ventricular thrombi may occur following a myocardial infarction.
The signs and symptoms of acute peripheral arterial occlusion vary with location. Large artery bifurcations seem to attract emboli more frequently than smaller ones. Arteries such as the femoral, iliac, and aorta are popular sites for occlusive disease. A recognizable pattern occurs when there is occlusion in an extremity. The onset may be gradual or abrupt; however, sudden onset of symptoms of pain with numbness, tingling, weakness, and pallor may signal peripheral emboli. Symptoms include pain, pulse, pallor, paresthesia, and paralysis. These five P's are the assessments of reduced arterial flow.
Intermittent claudication is frequently the only specific symptom of peripheral arterial disease. It reflects inadequate oxygenation of exercising muscle. Pain occurs only during walking and stops with rest. Patients describe either a tightening or pressing pain in calves or buttocks or a sharp, crampy calf pain. Most patients with arterial disease of the lower extremities are asymptomatic. Some patients complain of coldness in a foot.
Examination of peripheral pulses is the usual diagnostic method. Frequently a missing dorsalis pedis pulse is the first clue. The posterior tibial pulse is always present in persons without peripheral vascular disease, therefore if peripheral pulses are not palpable or found via the Doppler, peripheral vascular disease is suspected. The Doppler flowmeter is a machine that records ultra-high-frequency sound waves. When the transmitter is placed on the skin over an artery, the sound waves are beamed into the artery. If there is blood flow, the waves are recorded as a noise. Many patients with missing or absent peripheral pulses are asymptomatic. The clinical appearance of symptoms is the last stage of the pathologic process, which began years before.
When a patient complains of unilateral coldness or recent onset coldness, arterial insufficiency should be suspected. Numbness and paresthesia are also symptoms of peripheral arterial disease. Patients who describe numbness of toes rather than calf pain when walking should be suspect. This symptom occurs because of ischemia to peripheral nerves.
Rest pain in a foot is a symptom to be examined. It may indicate failure of collateral vessels to supply adequate blood flow to peripheral nerves and skin. The resultant ischemic neuritis produces the pain. It is described as burning, prickly, numbing, and becoming more prominent at night.
Careful palpation of pulses is the key to accurate diagnosis. The femoral pulse and the popliteal, posterior tibial, and dorsalis pedis pulses should be evaluated.
Assessment of the foot is important. With decreased cutaneous flow capacity, the foot tends to blanch on elevation above the heart level; the blanching is best seen on the plantar surface of the foot. Blood pressure comparisons in all of the extremities is also a clue when diagnosing peripheral artery disease. Blood pressure in both legs should be the same.
Rubor on dependency is a sign of severe ischemia. With advanced ischemia, ulcers and gangrene may occur.
Following diagnosis, vasodilating drugs may be ordered to improve blood flow. Agents include
Nursing ManagementPriorities for nursing care of a patient with peripheral arteriosclerosis are:
Nursing Diagnoses Most Frequently Associated with Peripheral Arteriosclerosis
|
Arteriosclerosis obliterans, the occlusive disease of the terminal aorta and common iliac artery, is the major cause of aortoiliac disease. Intimal plaques form, calcify, and become brittle and irregular, creating turbulent flow. As the plaques enlarge, the diameter of the lumen of the artery decreases.
The exact mechanism of development of arteriosclerotic obliterans is not clearly understood. Vascular stenosis develops slowly. The disease progresses to complete occlusion. Chronic aortoiliac disease usually is found in men aged 40-50 years. In women, surgically produced early menopause is a factor. Postmenopausal women also develop chronic occlusive arterial disease.
Hyperlipemia and diabetes mellitus are considered risk factors for the disease. A history of hypertension is also associated with arterial occlusive disease.
A gradual occlusion of an atherosclerotic terminal aorta and iliac artery causes ischemia to the distal parts in the periphery. Most frequently, the terminal aorta is affected, leading to obstruction and pressure in the smaller arteries distal to the obstruction. Blood flow declines and thrombosis can occur. If cellular deprivation occurs, gangrene may follow when the critical oxygen supply is short.
Because of the proximal location of aortoiliac disease, there is a potential for collateral circulation to bypass obstruction. As a result, serious cutaneous ischemia is unusual. Mild to moderate pallor on elevation is the only finding other than pulse deficits. An occasional, rare gangrene may occur.22 Dependent rubor or gangrene indicates distal disease. Coldness or sensitivity to cold is a frequent symptom and may be accompanied by color changes such as blanching or cyanosis.
In progressive aortoiliac disease, the femoral pulses are absent or very weak. The classic symptom is Leriche's syndrome (Chapter 7 p. 81), consisting of bilateral intermittent claudication and, in males, impotence. Pain is usually in hips and buttocks but varies in patients. Some patients describe only calf claudication. Some present with complaints of fatigue in hips and lower back on walking. Aortoiliac disease is frequently confused with herniated lumbar disc, osteoarthritis, osteoporosis of the lower spine, poor physical condition, and other problems.
Therapy is dependent on symptoms and their severity. Bypass surgery (Chapter 11) may be considered if severe claudication interferes with the patient's quality of life. Aortoiliac, aortofemoral, axillofemoral, and crossover femorofemoral bypass grafting are all possibilities.
Nursing ManagementPriorities for nursing care of a patient with aortoiliac disease are:
Nursing Diagnoses Most Frequently Associated with Aortoiliac Disease
|
Femoropopliteal occlusion tends to develop later than aortoiliac disease. Symptoms usually appear later in life. It is an extension of aortoiliac disease and usually follows the earlier atherosclerotic process.
Atherosclerosis occurs throughout the arterial system; lesions tend to develop at points of branching, bifurcation, curvature, or vascular narrowing. A common site is at the femoropopliteal vessels. The chronic occlusive disease progressively narrows the arterial lumen; this in turn increases resistance to blood flow and decreases tissue perfusion. Oxygen demand exceeds the ability of the vessel to supply oxygen, and ischemia occurs. One lesion can decrease the vessel lumen by 50%.
Diabetes is the major risk factor. Another common cause of femoropopliteal disease is atherosclerosis. Patients under age 55 with this disease are usually all diabetics and/or hyperlipidemics.22
Patients are asymptomatic until a serious defect occurs in blood flowing to the foot. The primary symptom of femoropopliteal disease is intermittent claudication due to muscle ischemia. Pain occurs with exercise and is closely correlated with the site of the arterial occlusion. Diagnosis is related to assessing a normal femoral pulse and absent or weak popliteal, posterior tibial, and dorsalis pedis pulses.
The treatment is dependent on the degree of foot ischemia. Surgery is indicated if there is (1) severe ischemia of the foot; (2) disabling intermittent claudication; and (3) nonhealing ulcers. Femoropopliteal surgery is then the procedure of choice.22
The nursing management is the same as for peripheral arteriosclerosis, page 86.
Raynaud's phenomenon and Raynaud's disease are often confused, causing misdiagnosis. Raynaud's phenomenon may occur in association with systemic disease. If no other cause is identified and the episodes (described later) persist, the condition is referred to as Raynaud's disease.
The manifestations for both conditions are similar, with skin color changes progressing from pallor to cyanosis to rubor. A vasospastic attack produces the changes. The first color change is pallor due to vasoconstriction of the small vessels. Cyanosis follows when dilation occurs in the vessels and oxygen is released. Rubor follows with restoration of blood flow. Rainbow phenomenon is the name given to the rapid color change in the fingers. Pain, cold, and numbness are the accompanying symptoms. The fingers quickly return to normal color after the rubor stage, when precipitating factors are removed, either by warming the hands or by removing the stressful event.22, 26, 28
The etiologic factors related to Raynaud's phenomenon can be divided into (1) hyperactivity of the sympathetic nervous system; (2) hypersensitivity of digital arterioles; and (3) sludging of elements of circulation.
In the first category, hypothyroidism has recently been recognized as a cause of Raynaud's phenomenon. The mechanism of Raynaud's in hypothyroidism is not clearly understood. A lowered metabolic rate may lead to vasoconstriction and decreased blood flow.22, 26, 41
Arteriolar hypersensitivity, the second category of etiologic factors, includes digital trauma, which may produce the localized Raynaud's phenomenon, collagen diseases/and scleroderma. The collagen diseases represent a major cause of Raynaud's phenomenon. Both systemic lupus erythematosus (SLE) and rheumatoid arthritis may be associated with this syndrome early in their course. Patients may develop Raynaud's as the first symptom of SLE; there may be years between this first symptom and development of SLE. With rheumatoid arthritis, the patient may have mild joint disease and severe vasospasm.
Scleroderma is the classic setting for Raynaud's phenomenon. This is a disease of unknown etiology, with progressive fibrosis and atrophy occurring in subcutaneous tissues, leading to adherence of the skin. The first sign of scleroderma is usually Raynaud's phenomenon. It usually predates other signs and symptoms by several years. Even if color changes do not occur, the hands are usually cold and sweaty. Cyanosis is easily precipitated by cold.22, 26
The third factor in the etiology of Raynaud's phenomenon is related to sludging of circulatory factors.22 Serum proteins that precipitate at low temperatures are at fault, as are fibrin split products found in the patient with disseminated intravascular coagulation (DIC). Raynaud's may occur as a result of either of these products or a combination of both. The exact mechanism is not clearly understood.
Blood flow studies (plethysmographic) reveal virtually no measurable blood flow in the digits of severely vasoconstricted individuals, but the digits do not develop intense pallor or cyanosis. The difference that creates the color changes in Raynaud's is not clear. It may be that there are immeasurable small differences in blood flow between normal individuals and those with Raynaud's phenomenon on exposure to cold.
Raynaud's phenomenon is associated with scleroderma. Survival of the patient rests with the course of the disease and the involvement of internal organs, especially in those patients with renal disease. Patients may have Raynaud's and severe visceral involvement.
The hands of a patient with Raynaud's phenomenon tend to be cool and sweaty, even at room temperature. The hands may change color during emotional tension. Long-standing disease may produce sclerodactyly, in which the digits become adherent to underlying tissue through fibrosis. Symptoms vary:
Some patients present with a mild feeling of coldness in the hands, and others have pain and numbness. Some patients have severe pain during color changes.
Diagnosis is made by the color changes or by cool hands associated with sclerodactyly. Confirmation of the diagnosis may be made by immersing the patient's hands in ice water if there is doubt.
There is no effective treatment for scleroderma. Vasodilators bring some relief from the problem of Raynaud's phenomenon. The treatment of Raynaud's phenomenon involves simple measures and drug therapy. Keeping warm is the high priority. Not only the hands and the feet but also the entire body should be protected. The warmer the body, the less reflex vasoconstriction. Vasodilator drugs are often given for severe arteriospasm in very cold times of the year. Some patients need the vasodilator agents all year because even bathing or dishwashing produces attacks. Drug therapy begins with low doses. Patients with scleroderma may require more vigorous vasodilatation.19, 22
Other medications used are the antihypertensives—the postganglionic blockers such as methyIdopa and guanethidine. Hypotension is an added risk in this therapy.
In some severe cases of Raynaud's, intra-arterial injection of reserpine has been used. Remission occurs for several months, but the reason why this is effective is not known. Beta blockers increase frequency and severity of attacks and should be avoided. Cervical sympathectomy, a surgical approach, has been used in treatment, but it is not a lasting cure.
The most common form of Raynaud's phenomenon is of unknown etiology and is called Raynaud's disease. This disease is more annoying than dangerous. Rarely do patients develop ischemic ulcers or atrophy of the fingers. This disorder is not associated with systemic disease and has an excellent prognosis.
Pathogensis is still questionable. The problem centers around whether the increased tendency to vasospasm is a primary disorder of the autonomic nervous system or hypersensitivity of digital arterioles. The presence of migraine headaches or hypertension in some of these patients can fit with either theory. The heightened sensitivity to cold does not explain attacks following stress.
Spasm causes the fingers to become pallid when they are cold. Blood cannot enter the capillaries. The capillary blood becomes stagnant in dilated vessels, releasing hemoglobin in larger than normal amounts; this causes the blue, cyanotic color change. Hyperemia and throbbing pain occur. The fingers tingle and frequently swell. The arteries of the fingers respond with vasoconstriction. This reddens the fingers for a brief period.
Diagnosis of Raynaud's disease is by exclusion of other disease processes. The distinction between the disease and the phenomenon relies on history.17, 22 Raynaud's disease is seen almost exclusively in otherwise healthy young women between the ages of 18 and 40 years. The onset is gradual; usually the first symptoms occur while the woman is in her early teens. An attack is usually precipitated by exposure to cold or by a strong emotional occurrence. Raynaud's disease is considered a primary disease, not associated with other peripheral vascular diseases. Simple treatment brings successful response. This disease is five times more common in women than men.
Buerger's disease, an inflammatory arterial dysfunction resulting in thrombus formation, has a definite link to males who smoke. This dysfunction occurs in the small- and medium-sized peripheral arteries in the foot and lower leg. Buerger's disease rarely extends to the arms, although it often extends to include adjacent veins in the legs.
Thromboangiitis obliterans is a disease of unknown etiology, most common in young men between the ages of 20 and 45. Heavy smokers are prime candidates. Some believe that tobacco is an etiologic factor, but opinion seems to be that it is only contributory. Recent research is directed toward immunologic studies. Recent reports of a cell-mediated sensitivity to human collagen in patients with Buerger's disease is encouraging.1
Buerger's disease is characterized by inflammatory thrombosis formation. As the disease process worsens, pain and gangrene of the extremities may occur. The disease usually affects the arteries of the leg below the knee, the popliteal arteries, and extends downward to involve branches and small digital vessels. Veins in the lower extremities also become involved as the disease progresses. Generally, the affected vessels may show areas with early inflammatory changes. In later stages, endothelial cells proliferate with thrombosis within the lumen of the vessel. There is a characteristic cordlike appearance to the disease segment of the vessel.
Pain and coldness are the primary symptoms of Buerger's disease. Early in the disease, intermittent claudication is reported. As the occlusion progresses, peripheral ischemia also produces pain at rest. Impaired circulation increases sensitivity to cold, nonhealing ulcers occur, and peripheral pulses become diminished or disappear completely. Color changes of the extremity are frequently noted with advancing disease. Frequently reported are cyanotic extremities in the dependent position and a reddish-blue color in the toes when nondependent positions are assumed. Buerger's disease will ultimately result in gangrene as tissues ulcerate with occluded vessels.
Diagnosis is by angiography, history, and appearance. Angiography shows a fairly normal peripheral vasculature to the level of the popliteal arteries.
Stenoses and occlusions appear in the popliteal arteries and their branches to the feet.1
Therapeutic Interventions
Cessation of smoking brings relief. In cases of ischemic ulceration, a mild vasodilator is prescribed.
Nursing ManagementPriorities for nursing care of a patient with arterial spastic disease are:
Nursing Diagnoses Most Frequently Associated with Arterial Spastic Disease
|
An aneurysm is an abnormal ballooning or dilatation of an artery wall produced by weakness in the vessel wall. Aneurysms may be small and localized or large and diffuse. Aneurysms are manifested in several forms. Classification is according to type and anatomic features.
A true aneurysm is one in which an intact arterial wall encloses a dilatation. A false aneurysm is a pulsating hematoma on the outside of the artery wall. A sac forms, communicating with the artery.
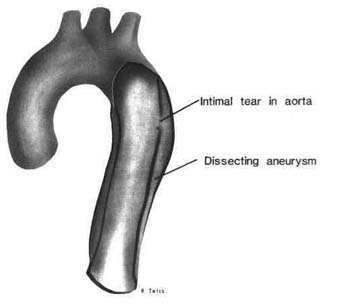
A sacular aneurysm is an outpouching of one side of an artery with a small portion adherent to the artery wall. It is thought to be caused by localized stretching of the medial layer. Fusiform aneurysm is a uniform circumferential dilatation with tapering at each end. A dissecting aneurysm (Fig. 8.2) is one in which a separation occurs in the arterial layers, forcing blood between the layers to accumulate in the medial layer. This aneurysm follows a tear in the intima. The site of an aneurysm may be the aorta or branches of peripheral arteries, such as the femoral or popliteal. The aorta is the most common site, with the thoracic and abdominal aortas the common areas of aneurysm development.4 Aneurysms are most common in the terminal portion of the abdominal aorta because of its sharp bifurcation into the iliac arteries. Frequently, the entire bifurcation of the aorta and the proximal common iliac arteries are involved. The sharp angulation of this segment produces turbulent blood flow over a relatively long segment. Abdominal aortic aneurysms are usually fusiform rather than saccular.5, 21
|
|
Figure 8.2 Dissecting aneurysm. |
The process of aneurysm formation usually is an exaggeration of the aging process in which smooth muscle and elastic tissue in the medial layer of the vessels are gradually replaced by atheromatous plaque. Stenoses and angular segments in the arteries accelerate the dilatation by creating pressure and turbulence at the site against the wall.4, 21
Before complications develop, the only finding is an expanding pulsatile mass. Once established, the aneurysm increases in size. As blood flows through the aneurysmal segment, forward velocity decreases and turbulence increases. The resultant thrombus formation and increased pressure on the wall causes further dilatation. This process may continue until rupture or development of serious thromboembolic problems.21
Complications are dependent on size and location. An extended aneurysm may produce problems in the renal, iliac, or mesenteric arteries. Internal blood pooling may produce thrombi or emboli. Rupture is always a possible complication. A further complication is emboli that detach from the mass.
Clinical manifestations depend on location and shape of the aneurysm. Symptoms, if present, reflect compression, erosion, rupture, or dissection of the surrounding structures. A thoracic aneurysm may produce cough, dysphagia, or hoarseness from tracheobronchial compression, pressure on the esophagus, or the recurrent laryngeal nerve. Abdominal aneurysm may produce pain from pressure on the spine or intercostal nerves. Abdominal aneurysms are frequently asymptomatic, detected only by radiology following a palpated pulsatile mass.
Dissecting aneurysms often mimic an infarct with severe chest pain and changes in tissue perfusion as the aortic branches are obstructed by the blood. The location of pain, described as "tearing," indicates the point of dissection (Fig. 8.2). Anterior chest pain points to the ascending aorta. Pain referred to the back is associated with dissection of the descending aorta. Severe hypertension usually occurs as the dissection continues and both pulse and blood pressure disappear as the arterial blood flow to the arms is occluded.
Peripheral aneurysms produce pain from pressure on nerve fibers. Peripheral thrombosis occurs in the blood pooled in the aneurysm's sac.
The majority of cases may be diagnosed by physical examination. Careful palpation of the abdominal aorta in a routine physical detects many aneurysms. The advent of abdominal sonography has made diagnosis of aneurysm safe, simple, and accurate (Chapter 16). Ultrasound delineates the anatomy of the abdominal aorta in detail.
The only effective method of treatment, when required, is resection and graft to restore arterial circulation.
Nursing ManagementPriorities for nursing care of a patient with aneurysm are:
Nursing Diagnoses Most Frequently Associated with Aneurysm
|
A thrombus is a mass of cellular material held together by a fibrin network that occludes a blood vessel. Phlebitis means inflammation of a vein;
phlebothrombosis means thrombosis of a vein, as does venous thrombosis. Thrombophlebitis means thrombosis and inflammation of a vein. Separating phlebitis and thrombosis is not clinically relevent because inflammation of the wall of a vein can lead to thrombosis, and clot in a vein can lead to vein wall inflammation.
Three major factors are involved in the formation of intravascular thrombosis: (1) vessel wall injury; (2) blood stasis; and (3) abnormal tendency for blood coagulation. Vessel wall trauma, as in contusions or fractures, often results in vessel wall injury. Table 8.1 lists additional predisposing factors.
Venous thrombi are usually formed in regions of slow or disturbed blood flow. They begin as small deposits in valve cusps or deep leg veins. Vein walls may be damaged by infections in soft tissue traversed by the veins. Intravenous infusions and irritating substances can cause injury. The continuous presence of an intravenous catheter can cause injury. Blood stasis in veins is a factor in intravascular coagulation. Stasis, inactivity, and immobilization during illness or following surgery are all factors that combine with sluggish venous blood flow to generate clotting.
| Table 8.1. Factors Predisposing Venous Thrombosis |
|
Characteristics of the blood itself contribute to stasis. The role of platelets and fibrin formation in the initiation of venous thrombosis is a factor. The altered state of the blood, which favors formation of venous thrombi, is referred to as a hypercoaguable state.
Deep vein thrombosis is an insidious disease because it usually displays no symptoms. A pulmonary embolus may be the first indication that venous thrombosis is present. Clinical symptoms are nonspecific, and the severity of the disease does not correlate with the fact that there are no signs or symptoms. The most reliable sign is swelling and edema of the involved extremity. Pain is the most common symptom reported. It is described as aching or throbbing; it can be mild or severe and accompanied by tenderness in the involved extremity. Walking may aggravate the pain.
Other signs that may be present include increased tissue turgor with swelling and increased skin temperature.
The physical examination, combined with signs and symptoms of superficial thrombophlebitis, is usually diagnostic. The veins are usually visible. Venography is usually not required for diagnosis. A varicose vein is often a major predisposing factor. A linear cord, approximately even in diameter, usually tender, reddened, and warm to the touch and located along a superficial vein, is strongly suggestive for diagnosis. Edema may also be present. Lymphangitis and cellulitis may occur in cases with venous valvular insufficiency, stasis dermatitis, and ulceration.
Contrast venography is considered to be the study most likely to determine the presence of deep venous thrombosis.
Varicose veins are dilated, tortuous, superficial veins of the lower extremities (saphenous veins).
Dilatation occurs as a weakness, acquired or congenital, of the vessel wall. The problem results from varying degrees of valvular incompetence. Varicose veins can frequently be traced to women who have undergone several pregnancies, and they also occur in older individuals.
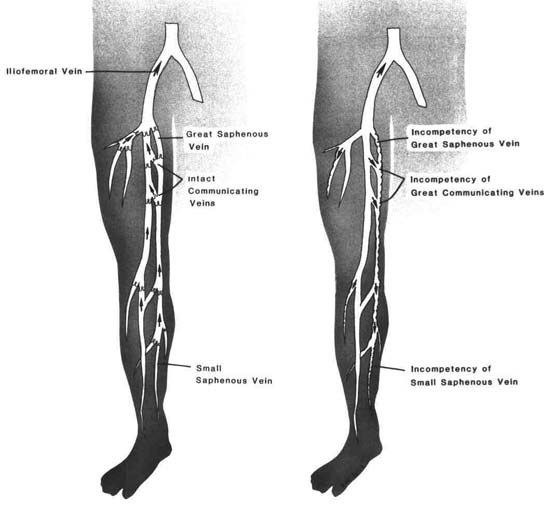
Blood volume, and therefore pressure, increases in the superficial venous system when valves are incompetent. Dilatation follows the venous stasis (Fig. 8.3). Primary varicosities result from problems within superficial saphenous veins, and secondary varicosities reflect a problem with impaired flow and dysfunction somewhere in the deep venous system.
Varicosities are clinically significant when the venous dysfunction is severe, when thrombosis occurs, or when stasis ulceration occurs. Frequently, the condition is of minimal concern, with slight discomfort and slight edema. Venous engorgement is usually the first evidence of varicosities.
Varicose veins become clinically significant when venous emptying is impaired. The venous insufficiency that follows produces a feeling of progressive heaviness from prolonged standing. At a later stage, edema and impaired tissue nutrition may occur. Ulcers, termed varicose or stasis ulcers, are an extension of the impaired venous circulation. The vascular insufficiency contributes to the chronic state of these ulcers, which heal very slowly. Stasis dermatitis, a condition in which the skin of the legs is edematous, with brown, irregularly pigmented, thin, shiny areas, may be a precursor to ulcer formation. Stasis dermatitis and ulcers occur most frequently on the lower part of the leg. Elderly patients are at the greatest risk.
Symptoms described are calf aching and heaviness, muscle cramps, and fatigue. Elevation of the legs usually brings relief. As the problem increases, dependent edema is evident with skin pigmentation occurring occasionally as a result of the venous stasis.
If treatment is required for symptoms, it is surgical (Chapter 11). Discomfort is relieved by leg elevation and support hose. Venous stasis may be relieved with support hose, but caution must be exercised with all types of stockings to avoid a tourniquet effect. Venous stasis is improved with active and passive leg exercises to stimulate blood flow. Injection of a sclerosing agent may be considered for small, asymptomatic varicosities.
Nursing ManagementPriorities for nursing care of a patient with thrombophlebitis or venous dysfunction are:
Nursing Diagnoses Most Frequently Associated with Thrombophlebitis or Other Venous Dysfunction
|
|
Figure 8.3 Common sites of varicose veins. |